
In this Article
Hyperthyroidism
What Is Hyperthyroidism?
Hyperthyroidism is a condition in which there is overproduction of thyroid hormone by the thyroid gland, causing the levels of thyroid hormone in the blood to be too high. People who have it are often said to have an “overactive thyroid”.

- The thyroid gland is a small, butterfly-shaped organ located in the neck below and in front of the Adam’s apple.
- Thyroid hormone is a chemical substance produced by the thyroid gland and released into the bloodstream. It interacts with almost all body cells, causing them to increase their metabolic activity.
This abnormally high level of thyroid hormone typically speeds up the body’s metabolism. Metabolism is the chemical and physical processes that create the substances and generate the energy needed for cell function, growth, and division.
Symptoms of hyperthyroidism may include a rapid heartbeat, tremor of the fingers and hands, weight loss, and the inability to tolerate heat.
|
Nice To Know: About the thyroid gland The thyroid lies just under the Adam’s apple in the neck. There are two lobes to the gland, and they lie just in front and at either side of the windpipe (trachea). The thyroid is part of the body’s endocrine system, which consists of glands that secrete hormones into the bloodstream. The thyroid gland secretes thyroid hormones, which control the speed at which the body’s chemical functions proceed (metabolism). To produce thyroid hormones, the thyroid gland needs The thyroid gland also produces a |
What Is Thyroid Hormone?
Hormones are chemical messengers released into the bloodstream by specialized glands called endocrine glands.
The hormone circulates through the body in the bloodstream delivering a message to other parts of the body. The “message” causes effects far from the gland that produced the hormone.
Thyroid hormone is produced in the thyroid gland, which is located in the front of the neck. It is released by the thyroid gland into the bloodstream and circulates throughout the body. Almost every cell in the body, from those in the brain to those in the feet, responds to the hormone.
There are two different forms of thyroid hormone present in the bloodstream. The two forms of thyroid hormone differ in the number of iodine units or molecules attached to the hormone. Iodine is a very important component of thyroid hormone.
- Thyroid hormone with four iodine units is abbreviated as
T4 . - Thyroid hormone with three iodine units is abbreviated as
T3 . - Most thyroid hormone in the blood is T4.
- T3 is the form that is active in the body, not T4.
- Certain cells in the body convert T4 to T3.
|
Nice To Know: Just about all the iodine we consume in food is used for the production of thyroid hormone. Iodine is added to regular table salt to ensure that individuals get enough iodine in their diets. Salt boxes are usually labeled “iodized salt.” People with deficiency in iodine will develop For more information about hypothyroidism, go to Hypothyroidism. |
For further information about hypothyroidism, go to Hypothyroidism.
What Does Thyroid Hormone Do?
Cells respond to thyroid hormone with an increase in metabolic activity. Metabolic activity, or metabolism, is a term used to describe the processes in the body that produce energy and the chemical substances necessary for cells to grow, divide to form new cells, and perform other vital functions.
If you think of each cell in the body as a car, then
Because thyroid hormone stimulates cells, it causes major body functions to “go” a bit faster.
- Heart rate increases.
- Breathing rate increases.
- Use of proteins, fats, and carbohydrates increases.
- Skeletal muscles work more efficiently.
- Muscle tone in the digestive system, such as those in the walls of the intestines that help to move food through the digestive system increases.
- Mental alertness and thinking skills are sharpened.
How Are Blood Levels Of Thyroid Hormone Controlled?
Normally, the body runs like a car on cruise control-functioning at a steady rate. This steady state is known as
- Special “detector” cells in the brain monitor the level of thyroid hormone in the blood.
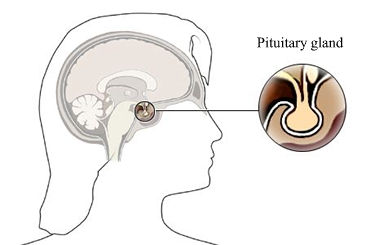
- When the level of thyroid hormone drops, these cells send signals to a nearby organ in the brain known as the
pituitary gland . - These signals stimulate the pituitary gland to release a substance called thyroid-stimulating hormone (TSH) into the bloodstream.
- TSH signals cells in the thyroid gland to release more thyroid hormone into the bloodstream.
- When the blood level of thyroid hormone has increased enough, the detector cells in the brain detect the increase in thyroid hormone level.
- These detector cells send signals to the pituitary gland to stop release of TSH.
|
Nice To Know: The medical specialty called |
|
What Causes Hyperthyroidism?
These are two major causes of hyperthyroidism.
- About 95 percent of persons diagnosed with hyperthyroidism are found to have a condition called Graves’ disease.
- Most of the remaining persons have a condition called nodular thyroid disease.
- A less frequent cause is inflammation of the thyroid gland, called thyroiditis
- Uncommon causes include
hormone producing tumors of thepituitary gland or ovary and iodine-induced hyperthyroidism from iodine-containing drugs
What Is Graves’ disease?

The immune system is a complex network that normally defends the body against “invading” organisms and other foreign substances. When the immune system detects a foreign substance in the body, it responds to this by producing antibodies against the invaders. These antibodies will recognize and attack this foreign substance when they next encounter it.
In Graves’ disease the immune system mistakenly directs an immune “attack” against its own healthy cells. Antibodies are manufactured and misdirected against the thyroid gland, mimicking the action of the hormone from the brain (thyroid stimulating hormone) that normally controls the thyroid function. These antibodies act like a switch put into a permanent “on” position. Thyroid cells are continually stimulated to produce and release
Any condition in which the body’s immune system attacks its own cells is called an autoimmune disease.
Graves’ disease is more frequent in women than in men. The symptoms of Graves’ disease may begin at any age but those between the ages of 20 and 40 are more likely to develop this condition.
What Happens With Graves’ Disease?
With time, the over stimulated thyroid becomes generally enlarged and may eventually become noticeable to the affected person or others as a swelling in the front of the neck. In addition, in some people Graves’ disease may be associated with particular eye and skin changes.
The eye changes are called hyperthyroid eye disease and occur in about 30 percent of people with Graves’ disease. These changes are visible as protruding eyes. There is no relationship between the appearance of eye changes and the severity of the hyperthyroidism. There is increased risk for infection and visual problems in persons with severe hyperthyroid eye disease.
Eye disease is most likely to progress in people who fit a certain profile. This includes those:
- Whose hyperthyroidism is not promptly corrected and controlled
- Whose thyroid hormone level is not within normal limits
- Who smoke cigarettes
The autoimmune process that causes hyperthyroid eye disease is poorly understood. Doctors do understand what causes the swelling of tissues behind the eyeball, decreased range of motion of the muscles around the eyeball, and retraction (a pulling back) of the eyelids.
Common symptoms include pain, excessive tearing, increased sensitivity to light, blurred vision, double vision, or protrusion of the eyes from the face.
The most common skin problem associated with Graves’ disease is called
What Is Nodular Thyroid Disease?
Nodular thyroid disease is unlike Graves’ disease in five important ways:
- Nodular disease is much less common.
- The cause is not known.
- It tends to develop in persons older than those who develop Graves’ disease.
- The disease process is not found throughout the thyroid gland.
- No particular problems outside the thyroid, such as eye or skin disease, are seen with nodular thyroid disease.
When a physical exam is done, the thyroid is usually enlarged and painless. As untreated disease progresses, distinct nodules (lumps) may be felt with the fingertips. Within the thyroid gland, nodules of abnormal thyroid cells are visible among areas of normal cells. This patter of nodular disease is seen as spots of over activity on
Is Hyperthyroidism Genetic?
Certain genetic factors may make someone more likely to develop an
Hashimoto’s thyroiditis , a thyroid condition that results in an unusually low thyroid hormone levelPernicious anemia
|
Nice To Know: The fact that there is a genetic basis for Graves’ disease means that more than one member of a family may develop it. When one person is diagnosed with Graves’ disease, other family members should have their thyroid function checked by their doctors. |
What Are The Symptoms Of Hyperthyroidism?
If you think of the body as a motor car, the most common symptoms of hyperthyroidism imitate a vehicle that is running too fast, for too long. These symptoms include the following:
- Rapid heartbeat, sometimes with palpitations
- Extreme tiredness
- Inability to tolerate heat
- Excessive sweating
- Weight loss, with a normal or increased appetite
- Nervousness and irritability
- Inability to sleep
- Shakiness and muscle weakness, often with trembling in the hands
- Diarrhea
- Menstrual problems in women, especially lighter periods or absence of periods
Some symptoms, such as excessive sweating and the inability to tolerate a hot environment are directly due to heat generated within the body by increased metabolic activity. Weight loss reflects use of body stores of fats, proteins, and carbohydrates, as normal food intake cannot keep up with demand.
The presence and severity of symptoms varies from person to person. For reasons not understood, older individuals with hyperthyroidism often have far fewe symptoms compared to younger people. Although many symptoms of hyperthyroidism cause distress, most are not dangerous. An exception occurs in some people who have heart disease. In these cases, untreated hyperthyroidism places additional stress on the heart, causing problems such as heart failure, irregular heartbeat (atrial fibrillation), or abnormal heart rhythm (arrythmia).
For further information about heart failure, go to Heart Failure.
For further information about palpitations, go to Palpitations.
How Is Hyperthyroidism Diagnosed?
Individuals with hyperthyroidism usually tell their doctors about symptoms such as rapid heart rate, intense fatigue, inability to tolerate a hot environment, and constant nervousness, jitteriness, or irritability. In addition, doctors look for physical signs such as weight loss, rapid heartbeat, slight tremors of the hands, or excessive sweating. The presence of such symptoms and signs strongly suggests the need for diagnostic testing for hyperthyroidism.
Hyperthyroidism is diagnosed from blood tests:
- Abnormally high levels of
T3 andT4 . This indicates that hyperthyroidism is present. - An unusually low level of circulating thyroid stimulating
hormone (TSH). This is normally due to an abnormality within thethyroid gland .
In some cases of hyperthyroidism, a special diagnostic scan of the thyroid gland using
RAIU testing shows whether:
- The entire thyroid gland is overactive, in which case, a large amount of radioactive iodine is “taken up” by the thyroid.
- Only portions of the thyroid are overactive. Significant amounts of radioactive iodine are “taken up” by portions of the thyroid, not the entire gland.
|
Nice To Know: Typically, |
How Is Graves’ Disease Diagnosed?
Most people with hyperthyroidism, or about 95 percent, are eventually diagnosed with Graves’ disease.
The diagnosis is confirmed through laboratory testing.
In people with Graves’ disease, blood tests usually demonstrate:
- Increased levels of T3
- Increased levels of T4
- Low levels of TSH
- Presence of thyroid stimulating antibodies
A radioactive scan, such as RAIU testing, is usually not necessary to confirm the diagnosis of Graves’ disease. If a scan is performed, it typically shows increased uptake of radioactive iodine throughout an enlarged thyroid gland. Areas of iodine uptake represent those areas in the gland producing
How Is Nodular Thyroid Disease Diagnosed?
When a physical exam is performed, the thyroid is usually larger than normal; however, there is usually no pain associated with an enlarged thyroid. As untreated disease progresses, individual lumps or nodules may be felt with the fingertips.
RAIU testing may be used to diagnose nodular thyroid disease. In individuals with this form of hyperthyroidism, this test shows clusters or nodules of abnormal thyroid cells among areas of normal cells. After this test, doctors see “spots” of overactivity on radioactive iodine uptake scanning film.
Is Hyperthyroidism Serious?
How serious hyperthyroidism is depends on the severity of the condition causing it. In people whose thyroid hormone levels are only slightly elevated, the symptoms will be fewer and less severe than for those with very high levels of circulating thyroid hormone.

The seriousness of hyperthyroidism also depends on how well the body can compensate for the changes brought on by excess thyroid hormones. For example, a heart that is already stressed by heart disease may deteriorate and develop heart failure as the heart rate rises in response to the increased level of thyroid hormone. In addition, serious eye complications are fortunately rare, but need to be properly cared for.
For further information about heart failure, go to Heart Failure.
How Is Hyperthyroidism Treated?
There is no known cure for Graves’ disease. Three forms of therapy are available for the treatment of hyperthyroidism.
These therapies work by decreasing the amount of thyroid hormone made by the thyroid gland; therefore, an excess amount of hormone does not get into the bloodstream.
The treatments available are:
- Anti-thyroid drugs
- Radioactive iodine, also known as radioiodine or 131I
|
How-To Information: When working with a doctor to decide the correct treatment for an individual, consider the following:
|
What About Surgery As A Treatment For Hyperthyroidism?
Surgical treatment for hyperthyroidism involves removal of almost all of the thyroid gland. The remaining part of the gland is not able to produce excessive amounts of thyroid hormone. This surgical procedure is known as a near total thyroidectomy. Surgical treatment is less common than in the past.

There are important points to know about surgery for hyperthyroidism:
- It brings rapid, permanent control of hyperthyroidism. Preparation before surgery with anti-thyroid drugs is advised; this may require several months.
- Almost all patients develop hypothyroidism following surgery.
- As with other surgical procedures, there are the usual risks of:
- General anesthesia
- Bleeding
- Nerve damage
- Wound infection
- Other type of infection
- Other complications
|
Need To Know: If any of the following factors are present, surgery is more likely to be recommended:
|
Possible complications of surgery
Preparation For Surgery
It is most important to have thyroid hormone levels under control before surgery. Achieving control of the hyperthyroidism before surgery avoids the risk of a “thyroid storm.” This condition, also known as a hyperthyroid crisis, is due to a failure of the body to tolerate hyperthyroidism in response to a stress, such as surgery.
- Preoperative, hormonal control is usually obtained with an
anti-thyroid drug , which partially blocks release of previously manufactured thyroid hormone from the overactive thyroid gland. - In addition, a few drops of an iodine solution are often taken daily for 10 to 15 days before surgery. These drops may decrease the size and number of blood vessels within the thyroid gland, thereby decreasing the risk for excess bleeding and other complications.
The Surgical Procedure
The operative procedure to treat hyperthyroidism is known as a near total thyroidectomy
- It is performed under general anesthesia.
- The surgeon makes an incision in the skin lines across the front of the neck and carefully exposes the thyroid gland.
- Precautions are taken to identify, isolate, and protect important structures in the area of the thyroid gland. Two are particularly important:
- The laryngeal nerve, which is vital for the proper function of the larynx or voice box, is carefully identified and protected from trauma during this procedure.
- The four small parathyroid glands, which are embedded in thyroid tissue and produce a
hormone necessary for maintenance of blood calcium levels, are also identified and preserved.
- Most of the thyroid gland is removed.
- The surgeon usually leaves about 3 to 8 grams, which is less the 0.3 ounces of thyroid tissue.
- The procedure generally takes several hours.
- The incision usually heals well and is usually not even noticeable.
Possible Complications Of Surgery
Thyroidectomy is considered safe, with a complication rate for injury to the laryngeal nerves or parathyroid glands of less than two percent. The rate of complications is lowest when an experienced surgeon performs the procedure.
Damage to one or more of the laryngeal nerves may result in changes of voice quality and tone. Damage to the parathyroid glands may cause problems with calcium balance.
Development of hypothyroidism or to a low level of circulating thyroid hormone is not considered a complication of the procedure, since it almost always occurs after surgery.
- The likelihood of hypothyroidism depends on how much thyroid tissue is removed during surgery.
- The likelihood of hypothyroidism depends on the underlying cause of the hyperthyroidism such as
Graves’ disease ornodular thyroid disease . - The risk for hypothyroidism is probably lower for individuals with nodular thyroid disease because the remaining tissue is likely to be normal.
- In individuals with Graves’ disease, the need to take enough tissue to make the risk of recurrence low normally results in hypothyroidism after surgery.
Medical Care After Surgery
Following surgery, patients are likely to remain in the hospital for one ot two days. After leaving the hospital, two types of follow-up are required. The individual needs to:
- Make a follow-up appointment with the surgeon to ensure that recovery is complete.
- Make an appointment with the endocrinologist to make sure that thyroid hormone levels decrease to normal and remain there.
If hypothyroidism develops, medical follow-up is important to make sure that an adequate thyroid hormone level is maintained with appropriate, ongoing thyroid hormone supplementation.
|
Need To Know: It is extremely important that people with hyperthyroid eye disease make sure that their thyroid levels remain normal after treatment for hyperthyroidism. Smokers must make every effort to quit. A smoking-essation program involving nicotine replacement therapy or a support group is usually helpful. For more information on how to stop smoking, go to Smoking: How To Stop. |
|
How-To Information: Long-term planning may involve various physicians, including a primary care physician, endocrinologist (specialist in disease of the glands), ophthalmologist (eye specialist), surgeon, or specialist in nuclear medicine. An individual with eye disease benefits when one physician, usually the endocrinologist, assumes responsibility for the collaboration among doctors. This is most likely to prevent a fragmented approach to treatment. In this way, doctors are able to coordinate treatment plans and implementation. For further infromation about how to stop smoking, go to Smoking: How To Stop. |
Hyperthyroid Eye Disease
Graves’ disease may be associated with particular eye changes.
The eye changes are called hyperthyroid eye disease and occur in about 30 percent of people with Graves’ disease. These changes are visible as protruding eyes. There is no relationship between the appearance of eye changes and the severity of the hyperthyroidism. There is increased risk for infection and visual problems in persons with severe hyperthyroid eye disease.
Eye disease is most likely to progress in people who fit a certain profile. This includes those:
- Whose hyperthyroidism is not promptly corrected and controlled
- Whose
thyroid hormone level is not within normal limits - Who smoke cigarettes
The autoimmune process that causes hyperthyroid eye disease is poorly understood. Doctors do understand that there is swelling of tissues behind the eyeball, decreased range of motion of the muscles around the eyeball, and retraction (a pulling back) of the eyelids.
Common symptoms include pain, excessive tearing, increased sensitivity to light, blurred vision, double vision, or protrusion of the eyes from the face.
Most people with hyperthyroid eye disease do not need any treatment beyond special eye drops. When more extensive care is required, treatments may be needed to decrease the pressure on the eyeball. This increase in pressure is the result of tissue swelling in the eye sockets. Additional treatment may be required to increase the range of motion (ROM) of the eyes or to improve the cosmetic appearance of bulging eyes. These may include:
- Treatment with certain drugs such as
steroids or immunosuppressive drugs to decrease the swelling behind the eyes. - External radiation therapy to decrease swelling behind the eyes.
- Surgery to remove a small portion of bone from the eye socket.
- Treatment with certain medications such as steroids or immunosuppressive drugs to help improve eye muscle function and increase range of eye muscle movements.
- Plastic surgery to improve the appearance of eyes or eyelids
|
How-To Information: When discussing treatment options, it is important to discuss several issues with your ophthalmologist including:
|
Looking After Yourself
People with hyperthyroidism may experience many uncomfortable and sometimes distressing symptoms. These may include:
- Weight loss
- Heart palpitations
- Anxiety
- Irritability
Before and during treatment for hyperthyroidism, make sure your doctor knows which symptoms or problem are most bothersome to you.
|
How-To Information: If anxiety or heart palpitations are troublesome, treatment with anti-adrenergic drugs, also known as beta-blockers, may calm these symptoms. If you already have heart disease, drug treatment with beta blockers may not be advisable. Be sure that your endocrinologist and other treating physicians are aware of your other medical conditions, if any. |
During treatment for hyperthyroidism, there may be some restrictions imposed on your day-to-day activities, including those related to your:
- Work
- Leisure time
- Recreational time
- Travel plans
This is particularly true for people who choose radioiodine therapy or surgery.
|
Need To Know: If antithyroid drugs or |
When treatment is complete, most people feel much better than before their treatment. They are able to do more and to enjoy the activities of their daily lives. Most find that, after appropriate treatment, there are essentially no treatment-related limitations on their activities of daily living.
The chance of developing
|
Need To Know: The possibility of lifetime hypothyroidism as a result of treatment for hyperthyroidism is real. Therefore, it is important to make a commitment to regular, lifetime follow-up care. This follow-up ensures that thyroid hormone levels remain normal. After thyroid hormone levels are normal and stable, it is possible that |
Hyperthyroidism And Pregnancy
About 1 in 500 women have hyperthyroidism during pregnancy. In some, it is a preexisting condition; in others, the condition will develop during the course of the pregnancy. It can be difficult to diagnose because the pregnancy often “masks” it; that is, some of the symptoms may be attributed to the pregnancy itself rather than to hyperthyroidism.
- Hyperthyroidism may affect a woman’s ability to become pregnant.
- The most common cause of hyperthyroidism in pregnancy is
Graves’ disease . - Symptoms generally will be worse in the first half of the pregnancy, will lessen during the second half, and most likely will recur after the baby is born.
- You should continue with your normal anti-thyroid medication during your pregnancy as prescribed by your doctor.
- Most pregnant women and their babies will not experience significant problems if the hyperthyroidism is mild to moderate. If properly treated the pregnancy can be expected to progress normally.
- Women with severe or uncontrolled hyperthyroidism have an increase risk of infection, iron deficiency (anemia), and high blood pressure accompanied by too much protein in the urine (a potentially dangerous condition called pre-eclampsia).
- If a woman has severe hyperthyroidism, her baby has a chance of having hyperthyroidism as well. There is a risk to the outcome of the pregnancy, having a small baby or a premature birth.
Fortunately, most women who have hyperthyroidism in pregnancy can be successfully treated with medication. The
Hyperthyroidism does not affect labor and delivery. However, thyroid storm can develop which can be life threatening. The symptoms are an exaggeration of the normal hyperthyroid symptoms with a very fast heart rate, tremors, nervousness, altered consciousness, nausea, vomiting, diarrhea, and an extremely high fever. This will require intensive care treatment to try normalizing the very high thyroid hormone levels and keeping the patient cool.
Following delivery, anti-thyroid treatment must continue. Although both the anti-thyroid drugs Propylthiouracil and methimazole do pass into the breast milk, both can be used safely in breast-feeding women. You should discuss this with your physician.
Your baby will be thoroughly checked to be sure he or she is well with no evidence of thyroid problems. Most babies born to hyperthyroid mothers whose hyperthyroidism has been well controlled during pregnancy are normal healthy babies.
Hyperthyroidism: Frequently Asked Questions
Here are some frequently asked questions related to hyperthyroidism:
Q: I was confused when I asked my doctor about my
A: There are two slightly different forms of thyroid hormone that circulate in the bloodstream. One form is abbreviated as T3, which is thyroid hormone with three attached
Q: I feel really sick with shakiness and have lost a lot of weight. The doctor who diagnosed my hyperthyroidism told me that I am a healthy 38-year-old man with hyperthyroidism. I know this condition can be treated, but how serious is hyperthyroidism?
A: Symptoms associated with hyperthyroidism, including your shakiness and weight loss, are distressing to many people with hyperthyroidism. However, for people like yourself who are generally healthy, treatment for hyperthyroidism usually proceeds as planned and eliminates these bothersome symptoms.
Q: I just learned I have
A: The fact that you, your cousin, and grandfather have Graves’ disease is probably not a coincidence. In some families, there is a genetic factor involved in the development of Graves’ disease or a tendency toward it and other autoimmune disorders. This may be true in your family. You and your cousin need to speak with other family members about Graves’ disease. Then, they can speak with their doctors and have their thyroid function checked.
Q: I was diagnosed with hyperthyroidism 11 years ago and treated with
A: Radioactive iodine is a safe and effective treatment for hyperthyroidism. It is the most common treatment for hyperthyroidism in the United States. In Europe, anti-thyroid medication, a non-surgical approach to the management of hyperthyroidism, is often the treatment of choice. There are benefits and risks to each type of treatment, and these vary depending on a person’s age, gender, and general health. If you feel fine and are maintaining proper follow-up with your doctor, don’t worry about your treatment choice.
Q: I have severe hyperthyroidism. Drug therapy didn’t work for me and I don’t like the idea of radioactive iodine. My doctor said that leaves surgery as the only option. The idea of somebody cutting into my neck really frightens me. How serious is this surgery?
A: Removal of most of the
Q: I just found out that I’m pregnant and I have Graves’ disease and hyperthyroidism. My obstetrician is setting up a consultation for me with an endocrinologist. What about pregnancy and hyperthyroidism?
A: Discuss all of your feelings and concerns with both your obstetrician and your endocrinologist. Take a team approach and have everyone work together to care for you during your pregnancy. You may need anti-thyroid medication during your pregnancy. Infants born to mothers who take anti-thyroid drugs generally have no drug-related complications. However, your thyroid hormone level will need to be monitored closely during your pregnancy. You will probably have to wait until after the baby is born to discuss your long-term treatment plan.
Q: A woman I know at work has a long history of Graves’ disease. I noticed that her eyes protrude from her face, now more than ever. I also know that she has trouble with blurred vision. Is there any treatment for this problem?
A: Hyperthyroid eye disease may be very troubling for individuals with Graves’ disease. Not only are there symptoms such as blurred vision, but there are also psychological complications due to the change in facial appearance. There are medical and surgical treatments available. If your friend hasn’t been evaluated by an ophthalmologist who is familiar with hyperthyroid eye disease, she should consider it. Severe hyperthyroid eye disease may be associated with increased risk for eye infection and other serious eye problems.
Q: I was treated for Graves’ disease and hyperthyroidism. I think that my current thyroid hormone level is fine. Should this have any impact on my future medical care?
A: Before your first meeting, doctors typically ask for a detailed medical, family, and drug history. Be sure to tell new doctors about your history of Graves’ disease. It is particularly important to know when your thyroid hormone level is high. The warning labels for some over-the-counter medications, including some for the common cold, contain warnings that persons with thyroid disease should check with their physician before taking any medicine. This warning is intended only for those whose thyroid hormone levels are high. It is possible that the medication speeds up the heart rate just like thyroid hormone does. This may lead to a potentially dangerous situation.
Hyperthyroidism: Putting It All Together
Here is a summary of the important facts and information related to hyperthyroidism:
- Hyperthyroidism is a condition in which there is overproduction of
thyroid hormone by thethyroid gland . - Symptoms of hyperthyroidism may include a rapid heartbeat, tremor of the fingers and hands, weight loss, and the inability to tolerate heat.
- The most common form of hyperthyroidism is Graves’ disease, a condition resulting from a problem with the body’s
immune system . Some families have a tendency toward developing Graves’ disease. About 95 percent of individuals with hyperthyroidism have this form of the disease. - About 30 percent of people with Graves’ disease have associated eye disease, which may cause significant changes in vision along with eyes that bulge or protrude from the face.
- The three major treatment options for hyperthyroidism-medication,
radioactive iodine , and surgery-work by decreasing the amount of thyroid hormone produced. - The effect of antithyroid drugs stops when treatment is discontinued, allowing the individual to switch to another treatment plan if necessary.
- Therapy with radioactive iodine permanently destroys thyroid tissue, meaning that too much thyroid will no longer be produced. The main disadvantage to this type of treatment is that
hypothyroidism (low levels of thyroid hormone) may result. However, hypothyroidism is treatable. - Surgery to remove almost all of the thyroid gland is called thyroidectomy and brings rapid permanent control of hyperthyroidism.
- Most people feel much better after treatment for hyperthyroidism is complete, but thyroid hormone levels still need to be checked periodically throughout a person’s lifetime.
- Most pregnant women and their babies will not experience significant problems if the disease is mild to moderate.
Hyperthyroidism: Glossary
Here are definitions of medical terms related to hyperthyroidism.
Adam’s apple: Part of the cartilage at the front of the neck that forms the larynx or voice box. It is more prominent visually and by touch in men than in women.
Anti-adrenergic drug: Any of a number of chemical agents that act to suppress the effects of adrenaline. One class is called the beta-blocking drugs.
Anti-thyroid drug: Any one of several chemical agents that interfere and hinder the production of thyroid hormone. Examples are propylthiouracil (PTU), methimazole (Tapazole®), and carbimazole.
Arrhythmia (of the heart): An irregular pulse or abnormal heartbeat.
Atrial fibrillation: Rapid, twitching contractions of one of the upper chambers or atrium of the heart.
Autoimmune disorder: Any one of a number of conditions caused by misdirected activity of the body’s own immune system. In people with an autoimmune disorder, the body mistakenly “attacks” its own healthy tissue.
Endocrine gland: A gland that releases a chemical messenger, known as a hormone, directly into the bloodstream that will affect other parts of the body. The thyroid is an endocrine gland.
Endocrinology: The study of the endocrine system and its associated activities. This is a very distinct subspecialty; a physician who practices in this area of medicine is known as an endocrinologist.
Graves’ disease: The most common form of hyperthyroidism or high levels of circulating thyroid hormone. Graves’ disease is an autoimmune disorder of the thyroid gland that causes excessive production and release of thyroid hormone. Hyperthyroid eye and skin changes are sometimes associated with this condition.
Hashimoto’s thyroiditis: An autoimmune disorder of the thyroid gland in which an immune response is misdirected against healthy thyroid hormone.
Homeostasis: A state of balanced function in the body.
Hormone: A chemical substance that is produced by an endocrine gland and released into the bloodstream to have its effect on other parts of the body. Also known as a “chemical messenger”. For example, thyroid hormone, released by the thyroid gland speeds up or stimulates certain bodily functions.
Hyperthyroidism: A condition characterized by a high level of circulating thyroid hormone. This may cause the “speeding up” of metabolic activity in body cells.
Hypothyroidism: A condition characterized by a low level of circulating thyroid hormone, causing inadequate stimulation of metabolic activity in body cells.
Immune system: A complex, organized system made up of special proteins, cells, and tissues that function to protect the body against disease-causing organisms such a bacteria or viruses; toxic substances or harmful chemicals; and foreign tissues, such as donor organs, or damaged cells. White blood cells are the primary cells of the immune system.
Immunosuppressive drug: Any of several chemical agents that decrease the function and activities of the immune system. In some cases, this class of drugs suppresses autoimmune activity. An example of an immunosuppressive drug is cyclosporine.
Iodine: A chemical element found in seawater and other sources. This chemical is necessary to produce thyroid hormone. Table salt labeled “iodized” contains added iodine and, for most people, is an important source of dietary iodine.
Metabolism: The chemical and physical processes that create the substances and generate the energy needed for cell function, growth, and division. Metabolism is also known as metabolic activity.
Nodular thyroid disease: A condition of the thyroid gland characterized by areas of overactivity within the thyroid gland. These areas are known as thyroid nodules. The exact cause of nodular thyroid disease, which may result in hyperthyroidism, is not known.
Nucleus: A round or oval structure inside a cell that regulates cellular activities. The nucleus contains genes, the units of heridity, that have a specific location on a chromosome. Genes are duplicated during each cell division. The function of a gene is to direct or “regulate” other proteins, including proteins that control body activities.
Ophthalmology: The study of the eye and its associated parts. This is a specialty in medicine and physicians who devote their practice to eyes and disorders affecting the eyes are called ophthalmologists.
Palpitations: An awareness that the heart is beating irregularly.
Pernicious anemia: A form of anemia or a less than normal level of circulating red blood cells. This condition is caused by an inappropriate autoimmune process that misdirects an immune response against the lining of the stomach. As a result, the stomach lining is damaged and vitamin B12 is not absorbed properly from food that is consumed. Vitamin B12 is necessary for proper red blood cell production.
Pituitary gland: A relatively small endocrine gland about the size of a pea. This gland is located underneath the brain and releases a number of essential hormones, including thyroid stimulating hormone (TSH).
Pretibial myxedema: A skin condition characterized by swollen, itchy patches of skin on the front of the lower legs or shins. This condition is associated with Graves’ disease.
Primary hyperthyroidism: A form of hyperthyroidism in which the disease process occurs within the thyroid gland itself. Graves’ disease is the most common form of primary hyperthyroid disease, followed by nodular thyroid disease.
Radioactive iodine: Iodine that contains a radioactive component. This element is chemically depicted as 131I. This form of iodine, which puts out intense energy, is used in a special test to diagnose thyroid disease.
Radioactive iodine uptake (RAIU) scanning: A special test used to diagnose thyroid disease. During this procedure, the amount of iodine “taken up” by the thyroid is measured and images or “pictures” of the thyroid gland are taken. So-called hot spots, or areas of particularly strong energy, represent areas of increased hormone production. Cold spots, or particularly weak energy spots, represent poorly functioning or nonfunctioning areas of the thyroid gland.
Retrospective: Literally, a look back in history. A “retrospective study” reviews the treatment of a disease over a period of time and the individual’s long-term response to therapy.
Steroids: A class of strong anti-inflammatory drugs that used to treat a variety of diseases, including certain autoimmune disorders.
Subtotal thyroidectomy: A surgical procedure during which part of the thyroid gland is surgically removed through an incision in the front of the neck.
T3: A term used to describe a form of thyroid hormone in the bloodstream. It has three units of iodine attached to the hormone structure. T3 is biologically active.
T4: A term used to describe a form of thyroid hormone in the bloodstream. This form has four iodine units attached to the hormone structure. Most thyroid hormone in the blood is T4; however, it is not biologically active in the body. Special cells convert T4 into T3.
Thyroid gland: A small, butterfly-shaped endocrine organ located in the neck below and in front of the Adam’s apple. The thyroid gland weighs about 20 to 25 grams and produces thyroid hormone, which is released into the bloodstream.
Thyroid hormone: A chemical substance produced by the thyroid gland and released into the bloodstream. It interacts with almost all body cells, causing them to increase their metabolic activity. Two forms of thyroid hormone, abbreviated as T3 and T4, are found in bloodstream.
Thyroid-stimulating hormone (TSH): A hormone produced and released into the bloodstream by the pituitary gland, which is located underneath the brain. TSH interacts with thyroid cells, causing them to produce and release thyroid hormone into the blood.
Thyrotoxicosis: Another name for hyperthyroidism or high levels of thyroid hormone. Term comes from prefix “thyro-” meaning thyroid, the root “toxic” meaning harmful, and the suffix “-osis” meaning condition.
Vitamin B12: A chemical substance found almost exclusively in meats. This vitamin is necessary for certain chemical processes in the body, including the ongoing production of red blood cells.
Hyperthyroidism: Additional Sources Of Information
Here are some reliable sources that can provide more information on hyperthyroidism.
Thyroid Foundation of America (TFA)
Phone: 800-832-8321
www.tsh.org
American Autoimmune Related Disease Association
http://www.aarda.org/
National
Phone: 828-877-5251
www.ngdf.org
American Thyroid Association
www.thyroid.org
Healthfinder, an Internet health information service developed in conjunction with the US Department of Health and Human Services.
www.healthfinder.gov
This site offers information in Spanish.