
In this Article
Hearing Loss
What Is Hearing Loss?
Hearing loss, or deafness, is the partial or total inability to hear sound in one or both ears.
The human ear is amazing. It is one of the smallest and most complex organs in the body, capable of turning the tiniest disturbances in air molecules into a form the brain can understand – and doing so instantaneously, over an enormous range of pitch and loudness. Considering the ear’s delicacy, it is remarkably resilient. Nevertheless, illness or injury can impair our ability to hear properly.
In recent years, substantial advances have made it possible to determine the cause of hearing impairment in nearly all cases, and to treat the hearing loss in many ears.
About The Ear
The ear is divided into three major parts:
- The outer ear
- The middle ear
- The inner ear

The outer ear has two parts:
- The trumpet-shaped, protruding part of the ear on each side of the head, called the auricle or
pinna - The tube leading into the ear, called the
auditory canal ; the opening is called the meatus

In the middle ear:
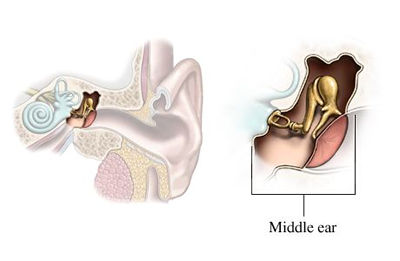
The
The middle-ear chamber is filled with air. There is an opening from the middle ear to the throat through a tube called the

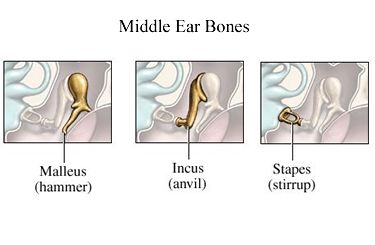
A chain of three small bones, called
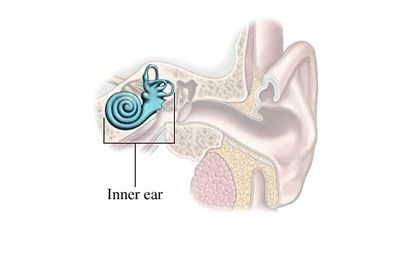
The inner ear is a fluid-filled chamber divided into two parts:
- The
vestibular labyrinth , which is the portion of the inner ear that functions as part of the body’s balance mechanism. - The
cochlea , which contains the hearing-sensing nerve.
The cochlea is a hollow tube inside the inner ear that is coiled to resemble a snail’s shell. It contains thiin fluid and a highly specialized structure called the
It is to the cochlea that sound vibrations picked up by the middle ear are carried.
The
How Do We Hear?
Hearing involves a complex chain reaction within the ear:
- Sound creates vibrations in the air somewhat similar to the rippling waves created when a stone is thrown into a pond.
- The outer-ear “trumpet” collects these sound waves, and they are funneled down the external ear canal to the eardrum.
- As the sound waves strike the eardrum, they cause it to vibrate.
- The vibrations are transmitted through the middle ear over the bony bridge formed by the hammer, anvil, and stirrup.
- These vibrations, in turn, cause the membranes over the openings to the inner ear to vibrate, causing the fluid in the inner ear to be set in motion.
- The motion of the fluid in the inner ear excites the nerve cells in theorgan of Corti, producing electrochemical impulses that are gathered together and transmitted to the brain along the acoustic nerve.
- As the impulses reach the brain, we experience the sensation of hearing.
The sensitivity of the hearing mechanism is most extraordinary. With the softest detectable sound, the eardrum only moves approximately one-millionth of an inch. Our ability to detect sounds from the softest to the loudest covers an intensity range of approximately 100,000,000 to 1.
What we hear are sound waves provided by vibrations of air molecules. The size and energy of these waves determine the loudness, which is measured in decibels (db). The number of vibrations or cycles per second makes up frequency – the more vibrations, the higher the pitch of the sound. Sound frequency is expressed in cycles per second, or hertz (Hz).
Many young, healthy humans (through teens and early twenties) can hear frequencies from about 20 Hz to 20,000 Hz, and can detect frequency differences as small as 0.2%. That is, we can tell the difference between a sound of 1000 Hz, and one of 1002 Hz.
Consequently, it is no surprise that such a remarkably complex system can be damaged by various illnesses and injuries.
How Does Hearing Loss Affect One’s Life?
Virtually no condition in medicine can have as profound an effect on quality of life as even moderate hearing loss in some people.
Hearing loss makes even routine communication difficult. High frequency hearing loss often involves loss of ability to hear consonants such as s, f, t, and z, even though vowels can be heard normally. Consequently, people hear but cannot make out what is being said.
This may result in frustration, withdrawal from social activities, depression, and marital discord. People lose the ability to take in the sounds like bird songs, rustling of leaves, and the voices of children. In general, these infringements on the quality of life can be overcome through medical or surgical treatment or with hearing aids.
When hearing loss occurs early in childhood, its devastating consequences are more obvious than when it occurs late in life. A hearing deficit in infants can interfere with psychological, emotional, and speech development. It also makes learning a mammoth task and can cause frustration or isolation.
Even more mild forms of hearing loss early in life can cause great difficulties, including poor attention and bad grades in school. Frequently, such children are considered “not too bright,” before anyone realizes that a hearing loss is present. When it is corrected, the changes in the child’s performance, attitude, and interactions are often remarkable.
|
Facts About Hearing Loss
|
Different Types Of Hearing Loss
There are different types of hearing loss, depending on which part of the hearing pathway is affected. A specialist will always try to localize where in the hearing pathway the problem lays, so as to be able to classify the hearing loss as belonging to one of the following groups. This is most important in determining the appropriate treatment.
They are:
- Conductive hearing loss
- Sensorineural hearing loss
- Central hearing loss
- Functional hearing loss
- Mixed hearing loss
We consider these below:
Conductive Hearing Loss
In cases of conductive hearing loss, sound waves are not transmitted effectively to the inner ear because of some interference in:
- The external ear canal
- The mobility of the
eardrum (problems with the mobility of the eardrum are often caused by accumulation of fluid in theeustachian tube , the tube that connects the middle ear to the back of the throat) - The three tiny bones inside the middle ear
- The middle-ear cavity
- The openings into the inner ear
- The eustachian tube
Modern techniques make it possible to cure or at least improve the vast majority of cases involving problems with the outer or middle ear. Even if people with conductive hearing loss are not improved medically or surgically, they stand to benefit greatly from a hearing aid, because what they need most is amplification.
Sensorineural Hearing Loss
In
The
- The term “sensory” hearing loss is applied when the damage is in the inner ear. Common synonyms are “cochlear” or “inner-ear” hearing loss.
- “Neural” hearing loss is the correct term to use when the damage is in the acoustic nerve, anywhere between its fibers at the base of the hair cells and the relay stations in the brain (the auditory nuclei). Other common names for this type of loss are “nerve deafness” and “retrocochlear” hearing loss.
|
Nice To Know: Sensorineural hearing loss is one of the most challenging problems in medicine. A large variety of hearing impairments fall under this category. Although the chances for restoring a sensorineural hearing loss are slim, a small number of cases can be treated, and some people experience dramatic improvements as a result. However, a great need for further research in this area still exists. |
Central Hearing Loss
In central hearing loss, the problem lies in the central nervous system, at some point within the brain. Interpreting speech is a complex task. Some people can hear perfectly well but have trouble interpreting or understanding what is being said. Although information about central hearing loss is accumulating, it remains somewhat a mystery in
A condition called central auditory processing disorder frequently leads people to think they have hearing loss when their hearing is actually normal. Despite the fact that this problem is extremely common and present in many highly successful people, it is actually classified as a learning disability.
Basically, the problem involves a person’s inability to filter out competing auditory signals. People with central auditory processing disorders have difficulties that include:
- Problems “hearing” when there are several conversations going on
- Inability to read or study with the radio or television on
- Problems reading if someone turns on a vacuum cleaner or air conditioner near them
- Generally missing the first sentence from people talking to them if they are involved in an auditory attention task (such as watching television)
Although such people (and their families and friends) frequently suspect that they have a hearing loss, the function of the ears is usually normal, and routine hearing tests are normal. Naturally, people with this condition may also develop hearing loss from other causes, and this can make it even more difficult for them to function under everyday circumstances.
There is no good treatment for central auditory processing disorders other than educating the person, family, and friends, and trying to control the environment. This is especially important for children, whose grades may go from F to A if they are provided with a silent place in which to do their homework.
|
Nice To Know: The test necessary to diagnose central hearing impairment must be designed to assess a person’s ability to handle complex information. Most of the tests now available were not created specifically for this purpose. It requires a very experienced and almost intuitive judgment on the physician’s part to make an accurate diagnosis. |
Functional Hearing Loss
Functional hearing loss involves a psychological or emotional problem, rather than physical damage to the hearing pathway. Individuals with this type of hearing loss do not seem to hear or respond; yet, in reality, they have normal hearing.
The most important challenge for physicians is to classify this condition properly. It may be difficult to determine the specific emotional cause, but if the classification is made accurately, the proper therapy can begin.
Too often, a functional hearing loss is not recognized, and individuals receive useless treatments for prolonged periods. In turn, this process may aggravate the emotional element and cause the condition to become more resistant to treatment.
Mixed Hearing Loss
Frequently, a person experiences two or more types of hearing impairment, and this is called mixed hearing loss. This term is used only when both conductive and sensorineural hearing losses are present in the same ear. However, the emphasis is on the conductive hearing loss, because available therapy is so much more effective for this disorder.
How Can I Tell If I Have Hearing Loss?
Hearing loss sneaks up on people. Often family members and friends are aware of hearing problems before the hearing-impaired person. Many people in the early stages of hearing loss of this sort will find themselves:
- Asking people to repeat themselves more frequently
- Offering inappropriate answers because they have misheard a conversation or question
- Going out less and socializing less
There are many other symptoms that may be related to hearing loss:
- Increased levels of frustration and irritability are common.
- Sometimes difficulty understanding speech is more of a problem than an inability to hear speech.
- Feelings of ear fullness or pressure, ear noises (ringing, buzzing, crickets, seashells, steam, and others), and dizziness.
Hearing loss is not always slowly progressive and stable from day to day. It may be sudden, rapidly progressive, or even fluctuating (good times and bad times).
What Should I Do For Hearing Loss?
If you think you have some hearing loss, you should see your doctor. Your primary care physician may refer you to a hearing specialist.
- Otolaryngologists (ear, nose, and throat doctors) are specialists in ear problems, among other things.
- Otology is a subspecialty of otolaryngology. Otologists have a special interest in and concentration on ear problems.
- Neurotology is a further subspecialty of otology. Although the field is more than 30 years old, there are relatively few physicians with experience and/or fellowship training beyond otolaryngology residency who qualify as neurotologists. Neurotologists specialize in the ear, and are specially trained to treat diseases of the inner ear and ear-brain interface, and to perform skull base and intracranial surgery.
- Otoneurologists are specialists whose background is in neurology and who have a special interest in disorders affecting hearing and balance. But their perspective and background is different from that of a neurotologist. They diagnose neurological problems related to hearing but do not perform surgery on the ear and related structures.
What Should I Expect From My Ear Doctor?
An ear doctor will want a complete history of the hearing problem. This will include information on:
- When it started
- How fast it progressed
- Whether there were obviously related problems (illness, head injury, noise exposure etc.)
- Whether other members of the family have hearing loss
- Whether there have been ear infections
The ear doctor will also ask about general health because of the numerous health conditions that may cause hearing problems.
The ear doctor will also perform a physical examination. Ordinarily this includes a complete ear, nose, and throat examination. An otologist usually includes an informal hearing assessment with a tuning fork, which is a small metal instrument that the doctor taps and holds near the person’s ear. Other assessments of balance, sensation, and other functions also may be performed.
A hearing test (
What Kinds Of Hearing Tests Are Done?
The various tests that may be performed for hearing loss include:
- Audiogram
- Tympanometry
- Site of lesion testing
- BERA
- Other types of testing
- Tests not directly related to hearing
We consider these below:
Audiogram
An audiogram is a hearing test that is generally performed in a soundproof room using sophisticated, calibrated equipment. A trained professional, most commonly a certified audiologist, usually administers the test. Earphones are placed over the person’s ears, and tones are presented to each ear, one at a time. The softest level at which the sounds can be heard is recorded.
Tympanometry
Tympanometry is a common test that involves placing a gentle pressure probe in the ear. This test assesses the pressure in the middle ear, and it may help detect fluid, problems with the middle ear bones, and other conditions.
Site Of Lesion Testing
Site of lesion testing involves the regular equipment used in an audiogram, with a variety of other tests to help determine where a problem lies. This kind of testing may involve:
- Comparing the hearing in one ear with the other
- Detecting small changes in signal intensity
- Testing ability to hear in the presence of noise
- Testing the ability to hear sentences placed in both ears at the same time
BERA
Brainstem evoked response audiometry (BERA or ABR) involves sophisticated, computerized equipment. Sounds are placed in the ear, and the brainstem’s response is recorded from electrodes (similar to electrocardiogram electrodes) that are taped to the patient’s head. This testing is extremely helpful in:
- Distinguishing sensory (inner ear) from neural (nerve) causes of hearing loss
- Helping to localize problems in the brainstem auditory pathway
- Determining the ability to hear soft sounds, in selected cases
Other Types Of Testing
A person experiencing ear noise (a condition called tinnitus) can be tested in several ways. Sometimes it is possible to measure the frequency and intensity of the
Since the inner ear is divided into hearing and balance sections that are related, balance system testing is often appropriate for people with
The most common balance tests are:
- Electronystagmography (ENG). ENG involves measuring eye movements and stimulating the body’s vestibular system, which controls balance. This kind of testing is not widely available, but it may be valuable for some people.
- Computerized dynamic posturography (CDP). CDP tests overall balance function using a computerized testing platform. It provides invaluable information that is especially useful in combination with an ENG.
Tests Not Directly Related To Hearing
Because of the complexity of the hearing system and the many things that may affect it, an evaluation of other parts of the body is often helpful. This usually involves blood tests and imaging studies. Imaging studies may include:
- A magnetic resonance imaging (MRI) scan to look at the inner ear nerves and brain
For more information about MRI, go to MRI.
- A computed tomography (CT) scan to look at the bones of the ear
For more information about CT Scan, go to CT Scan.
- Magnetic resonance angiography (MRA), or occasionally angiography, which produces images of the blood vessels to the brain
- A SPECT or PET scan, which produces images of microscopic blood flow within the brain.
What Causes Hearing Loss?
What problems can affect the outer ear?
What problems can affect the middle ear?
What problems can affect the inner ear?
We consider these questions below:
What Problems Can Affect The Outer Ear?
Anything that completely blocks the ear canal can cause hearing loss. Blockage with earwax (also called cerumen) is common. A doctor can cure this easily by removing the wax either with specially designed instruments or by flushing with water. There are many over-the-counter wax control preparations that can be used at home. However, they sometimes can cause external ear infections.
|
Need To Know Q: Is it a good idea to remove wax inside the ear with cotton-tipped swabs? A: No. The ear has a natural self-cleaning mechanism. Ear skin normally sheds from the inside out. If you place a drop of ink on the |
Many other problems can block the ear canal and lead to hearing loss. Such blocking causes a decrease in volume but does not generally produce distortion. These problems include:
- Infections with swelling that shuts the ear canal
- Foreign bodies in the ear
- An injury
- Birth defects
- A growth in the ear canal
Any of these, including blockage by wax, may result in
What Problems Can Affect The Middle Ear?
Problems that can affect the middle ear and lead to hearing loss include:
- Ear infections
- Fluid in the ear
- Otosclerosis
- Birth defects
- Tumors
Temporary hearing loss is commonly caused by ear infections. Middle ear infections cause swelling of the lining in the middle ear, and often an accumulation of fluid (such as pus). When there is fluid behind the eardrum and surrounding the
Infections are usually treated with antibiotics, sometimes with decongestants, and occasionally with drainage by placing a small hole in the eardrum (a procedure called myringotomy). If infections are severe or inadequately treated, they may cause permanent hearing loss by damaging the ossicles or perforating the eardrum.
|
Nice To Know: Most perforations (holes) in the eardrum heal spontaneously. When one does not, it can nearly always be repaired with surgery. The procedure is usually relatively fast, and is generally performed under local anesthesia. |
Glue ear
Ear fluid not caused by infection accumulates commonly in children, and sometimes in adults. The condition is known as glue ear, or chronic otitis media with effusion (OME). It sometimes requires drainage through a
Fluid in the ear usually is due to malfunction of the
- The eustachian tube does this by opening momentarily when we swallow or yawn.
- If it fails to open because of swelling, allergy, or other reasons, the air already in the middle ear becomes trapped.
- Gradually, this air is absorbed into the bloodstream. The middle ear space is bony except for the eardrum. As absorption occurs and less and less air is present, its disappearance creates a vacuum (negative pressure), which sucks the eardrum toward the middle ear (retracted ear drum).
- When the negative pressure is great enough, it causes fluid to seep out of the blood vessels that line the middle ear. This is the fluid that constitutes glue ear.
The presence of fluid causes hearing loss, and sometimes frequently recurring ear infections. In some cases, the eustachian tube starts to work again spontaneously and the condition resolves. In others, decongestants may be helpful. When allergy is the cause, allergy treatments may improve the problem.
When the condition causes frequent middle ear infections (acute otitis media) some physicians recommend the long-term use of antibiotics, although this treatment is currently controversial.
For more information about glue ear, go to Glue Ear.
For more information about middle ear infections, go to Middle Ear Infection.
Otosclerosis
Otosclerosis is a common hereditary disease in which new bone is deposited around one of the tiny bones in the middle ear, specifically around the footplate of the stapes (or ‘stirrup’) bone. This prevents normal bone transmission of sound from the eardrum to the inner ear, and consequently, conductive hearing loss results.
This hereditary condition is present in about 10 percent of white Americans, and it causes significant hearing loss in about one percent. It occurs less commonly in black and Asian people. Otosclerosis generally becomes apparent during early adult life, and the severity of hearing loss can be accelerated by pregnancy.
This type of hearing loss can be cured by a surgical procedure called stapedectomy, in which the stapes bone is replaced by an artificial bone. This procedure usually only takes 30 or 40 minutes, and it is performed under local anesthesia (in which the person is awake). In many cases, hearing can return to normal after surgery.
Various birth defects may also involve the middle ear and cause hearing loss. Some are major and cause obvious external defects. Many involve only the inner ear structures. In any case, most conductive hearing loss, in which sound waves are not transmitted effectively to the inner ear, is surgically treatable.
Tumors of the middle ear may be responsible for hearing loss. They may be cancerous (malignant) or noncancerous (benign).
- Examples of cancerous tumors are rhabdomyosarcoma, a very rare muscle tumor, in children or squamous cell carcinoma in adults.
- Examples of noncancerous tumors are glomus tumors (which also cause pulsating ear noises) or neuromas of the facial nerve.
- Cholesteatoma is a common noncancerous skin cyst that grows slowly and dissolves adjacent bone as it grows. It is a fairly common problem, especially in people who have had repeated ear infections; but it may also occur from birth. It generally requires surgery to remove the cyst.
What Problems Can Affect The Inner Ear?
There are many conditions that cause the delicate inner portion of the ear to function abnormally. They include:
- Otosclerosis
- Presbycusis
- Fistula
- Head injury
- Meniere’s syndrome
- Noise
- Infections
- Sudden deafness
- Neural problems
Otosclerosis (the hereditary disease in which bone deposits collect around the small bone in the middle ear known as the stirrup) can also affect the
The natural aging process also causes
There also are other age-related causes of hearing loss, including stiffening of portions of the cochlea and loss of nerve endings in the
A fistula (opening) is an abnormal connection between the inner ear and middle ear. The inner ear is filled with fluid, and the middle ear is filled with air. If a fluid leak occurs from the inner ear, hearing loss and dizziness commonly result. This kind of hearing loss often is cured by surgically repairing the fistula. Such leaks are usually caused by trauma. The trauma may be direct, such as a blow to the ear or a head injury in a car accident. However, it may also be the result of air pressure changes in an airplane trip, a forceful sneeze, or lifting a heavy object.
Direct head trauma, particularly trauma severe enough to cause unconsciousness, can cause inner ear concussions and hearing loss.
Meniere’s syndrome is a condition characterized by fluctuating hearing loss (usually more prominent in the lower frequencies where we hear speech), dizziness, fluctuating ear pressure, and
There are many treatable causes of Meniere’s syndrome. When all tests have revealed none of the known causes, the condition is classified as Meniere’s disease.
Noise is an important cause of hearing loss. An estimated 7 to 10 million people in American industry have noise-induced hearing loss, virtually all of which was preventable. In addition to industrial noise, recreational noise can damage hearing. Such noise is encountered commonly from gunfire, power tools, snow blowers, motorcycles, loud music (especially with earphones) and other causes.
In some cases, the playing of musical instruments can damage hearing. This has been reported not only with loud, electrical rock and roll instruments, but also with classical music performance such as violin playing and flute playing. One can minimize such problems by using ear protection whenever practical, such as during selected practice sessions.
Infections involving the inner ear and hearing nerve can also produce deafness. Middle ear infections can spread to the inner ear, causing loss of hearing and, usually, dizziness. Infections may also involve the hair cells or acoustic nerve, causing hearing loss and even sudden total deafness.
For more information about middle ear infections, go to Middle Ear Infection.
Sudden deafness may be caused by a variety of problems. Treatment is controversial, but there is some evidence to suggest that aggressive treatment may improve the chances for hearing recovery even after a sudden profound loss. Once the condition has been present for more than two or three weeks, even the most aggressive treatments generally do not work.
Neural (nerve-related) problems may also produce hearing loss. Among the more common are:
Acoustic neuroma , a common tumor of the acoustic nerve- Multiple sclerosis
- Autoimmune sensorineural hearing loss, in which the body attacks its own ear
- Ototoxicity, which is hearing loss caused by a substance that gets into the body; most often the substance is a medication, particularly certain antibiotics, but other toxins (such as lead) may also cause hearing loss

|
Need To Know: What is an acoustic neuroma? An acoustic neuroma is a common tumor of the acoustic nerve, the nerve responsible for hearing. It generally starts in the internal Ordinarily, these tumors can be cured with surgery. They are managed best by neurotologists, inner ear subspecialists with particular interest and expertise in treatment of this specific tumor. Neurotologists often work in collaboration with a neurosurgeon. In the majority of cases, it is possible to remove acoustic neuromas without serious injury and without facial paralysis. In some tumors diagnosed early, it is even possible to preserve hearing (despite the fact that the tumor has its roots in the acoustic nerve). |
What Other Conditions Can Cause Hearing Loss?
A number of other problems can cause hearing loss, particularly sensorineural hearing loss. Many of them are very common conditions that are not always associated with hearing loss. They include:
Common Childhood Infections
Mumps is the most common cause of one-sided total deafness in the United States. Frequently, the child and family are not aware of the hearing loss until years later. Other childhood infections, such as scarlet fever, may also affect hearing, particularly by destroying the eardrum and damaging the middle ear bones.
Special Infections
Many infections can result in hearing loss, including:
- Syphilis. It can be acquired at birth or through sexual contact, and a person may have it a long time before hearing symptoms occur (sometimes for 30 or more years). Caught early, this form of hearing loss can be cured. However, if it is not recognized and treated, the hearing loss may progress and even become total.
- Lyme disease. This increasingly common infection is spread through the bite of a tick. Lyme disease often causes a rash and joint pain, but these may be minor enough to escape notice. A diagnosis of Lyme disease can be made with blood tests. It is treated with antibiotics.
- Numerous other infections including herpes, cytomegalo virus (CMV), measles, mononucleosis, chickenpox, pneumonia, flu, and fungal diseases may cause hearing problems as well.
Problems With Blood Flow
Insufficient blood flow in the inner ear or related areas of the brain can contribute to hearing loss. This can happen as a result of cardiovascular disease, untreated high blood pressure, and other similar conditions. It also may be present in people whose blood tends to sludge and clot excessively (hypercoagulability), or who have too many blood cells (polycythemia).
Meningitis
Hearing loss is one of the most common consequences of meningitis, especially bacterial or fungal meningitis. Meningitis is an infection of the membranes covering the brain and spinal cord. Anyone who has had meningitis should have a hearing test upon recovery.
For more information about meningitis, go to Meningitis.
Tuberculosis
Tuberculosis and other similar illnesses have been associated with hearing loss. The problem may be due to the disease itself or to the medications used to treat the disease (such as streptomycin). Despite the availability of vaccines for tuberculosis, it is becoming increasingly common, especially among people with AIDS and those who come in contact with them.
Arthritis
Arthritis (inflammation of joints) and vasculitis (inflammation of blood vessels) commonly are associated with hearing loss. These include conditions such as rheumatoid arthritis, lupus erythematosus, and others. The hearing problem is probably related to abnormalities in blood vessels from these diseases.
Allergies
It is well recognized that allergic problems in children cause fluid to collect in the eustachian tubes and middle ear. However, in some cases allergies may also cause inner ear problems such as
High Blood Pressure
Some conditions associated with high blood pressure (such as hypolipoproteinemia, which is extremely high cholesterol and triglyceride levels in the blood) are also associated with hearing loss. In general, it appears that people with high blood pressure have a higher incidence of hearing loss. They may also be more prone to noise induced hearing loss than others.
For more information about high blood pressure, go to High Blood Pressure.
Thyroid Problems
Hypothyroidism (underactive thyroid) is commonly linked with hearing loss. About half of people with low thyroid function have hearing losses. Moreover, about 3% of people with Meniere’s syndrome have hypothyroidism; and in some, control of the thyroid disease eliminates the symptoms of Meniere’s syndrome.
For more information about hypothyroidism, go to Hypothyroidism.
Kidney Disease
Many of the things that damage the kidney also damage the ![]()
Cancer
Cancers that involve the ear and the brain can cause hearing loss. However, cancers elsewhere may also be related, particularly because many of the treatments for cancer produce hearing loss. Chemotherapy agents can affect the ear. Radiation may also cause hearing loss if the ear is included in the radiation field. Individuals who receive chemotherapy or radiation therapy should have an
Diabetes
Diabetes is one of the most common diseases in the United States. Although estimates vary from study to study, it appears that about 40 percent of people with diabetes have hearing loss. It usually occurs in both ears and is most severe in the high frequencies. However, Meniere’s syndrome may also be caused by diabetes, and sudden deafness can occur.
For more information about diabetes, go to Diabetes In Adults.
Glaucoma
The relationship has been controversial, but it is probable that there is a significantly increased incidence of hearing loss in people with glaucoma, a condition in which there is high pressure within the eye. This is especially true for people with a type of glaucoma called narrow-angle glaucoma.
For more information about glaucoma, go to Glaucoma.
Sickle Cell Disease
About seven percent to nine percent of black Americans carry the sickle cell trait. About 1 in 400 has sickle cell disease, and 20 percent to 25 percent of people with sickle cell disease have sensorineural hearing loss. Sudden deafness has also been reported in connection with this condition, although in some cases hearing will return.
Fainting Disorders
A person who has hearing loss (often severe) along with fainting may have a condition called Jervell and Lange-Nielson syndrome. This hereditary condition accounts for approximately 1% of all cases of hereditary deafness. If hearing loss and fainting occur together, a person’s heart should be checked immediately. The fainting can be due to heart arrhythmias (irregular heartbeats) that may cause sudden death.
Tinnitus And Dizziness
For more information about tinnitus, go to Tinnitus.
Hereditary Diseases And Syndromes
There are many hereditary diseases and syndromes that can lead to hearing loss. The syndromes involve defects in virtually any part of the body. Hearing loss is often hereditary.
- When it runs in families from generation to generation, the hearing loss usually follows a hereditary pattern called “autosomal dominant.”
- However, the absence of a family history does not mean that hearing loss is not genetic. “Autosomal recessive” inheritance is common. It means that neither parent has hearing loss, but both carry a gene that causes it. On the average, the hearing loss will be present in one child out of four.
How Is Hearing Loss Treated?
The first step in treating hearing loss is an accurate diagnosis – finding out exactly what’s causing the hearing loss. When a specific cause is found, treatment options can include:
- Treating the underlying disease, such as hypothyroidism, if a disease is found.
- A hearing aid to provide amplification of sound (for most people with sensorineural hearing loss, amplification is the best or only option)
- Surgery for mechanical causes such as chronic ear infections
How good are hearing aids?
What is a cochlear implant?
What should I know about ear surgery?
How Good Are Hearing Aids?
Hearing aids are never as good as perfect hearing. However, there have been dramatic improvements in technology. In general, it is possible to find a very satisfactory, appropriate hearing aid as long as there is some residual hearing (not total deafness).
Reputable hearing aid dealers, audiologists, speech and hearing centers, and some ear doctor offices dispense hearing aids. Any reputable hearing aid dispenser offers a 30-day return period, during which the hearing aid can be brought back for refund if the user finds it unsatisfactory.
|
Need To Know: Selecting a proper hearing aid requires skilled evaluation and testing with numerous devices and electronic adjustments. Door-to-door salespeople do not ordinarily have the capabilities to perform such testing and should generally be avoided. |
Hearing aids vary greatly in style and cost. Some fit almost entirely within the ear and are nearly invisible. A larger hearing aid that fits behind the ear may be necessary. Occasionally, for extremely severe hearing losses, traditional “body aids” with a wire are still used, but these are required for only a very small number of people.
Selecting a hearing aid is a very personal process, and it is essential that any potential hearing aid user have the opportunity to listen to a variety of instruments adjusted expertly before making a selection. Expensive, fancy digital hearing aids are now available. For many people, they really do offer substantially improved sound quality, and digital programming options that make it easier to hear with noise.
Hearing aids can be worn on one or both ears depending upon the hearing loss. There are even CROS (contralateral routing of signals) aids for total deafness in one ear, in which a microphone is placed on the deaf side and transmits sounds by radio signals to the good side. This is a great convenience for many people who have to function in meeting rooms. It is also extremely helpful when driving. For example, a person driving with a deaf right ear has trouble hearing a passenger, especially if the driver’s window is open.
What Is A Cochlear Implant?
A cochlear implant is a device that restores hearing to people with very severe or profound deafness. Cochlear implants have been used since the late 1960s.
A cochlear implant is a safe electronic device that is implanted beneath the skin and into the inner ear (in rare cases, the device can actually be implanted directly into the brain). Once the outer skin has healed, an external device is placed on the skin over the implanted device and turned on.
Cochlear implants allow totally deaf people to hear common sounds such has a telephone, doorbell, car horn, and spoken voice.
- In almost all people, understanding of speech is possible and lip reading is improved dramatically by the ability to hear the rhythms and the stops in normal speech.
- Most people are able to talk on the telephone with modern cochlear implants.
Until very recently, cochlear implants were approved for use only in people with profound (total or near-total) deafness. However, in 1995, the FDA approved expanded indications to include people with severe hearing loss as well. This change came about after an eight-year study that showed people with cochlear implant get better hearing than with traditional hearing aids.
What Should I Know About Ear Surgery?
Ear surgery is extremely common, and it is generally safe and effective when performed by an expert surgeon. Certain operations are particularly common:
Myringotomy and tube placement involves making a small incision in theeardrum , suctioning fluid out of the middle ear, and placing a ventilating tube within the eardrum. In children, the procedure requires general anesthesia. In adults, it can be done as an office procedure and ordinarily takes only a few minutes. After tubes have been placed, they generally fall out by themselves in 3 to 12 months. Most physicians agree that is important to keep the ears dry (avoid water) while the tubes are in.- Stapes surgery is performed under local anesthesia. Like all ear surgery, it requires the use of an operating microscope. The eardrum is moved aside, and the immobile stapes bone (the stirrup) is either mobilized or replaced with an artificial bone (usually made out of Teflon and stainless steel). As with all ear surgery, there are potential risks including worse hearing loss,
tinnitus , dizziness, facial paralysis (extremely rare), bleeding, infection, and others. However, the overall success rate of stapes surgery is in the range of 97% or 98%, and many people prefer surgical restoration of hearing to wearing hearing aids. - Tympanoplasty and Mastoid surgery usually involves general anesthesia (although it can be performed under local anesthesia when necessary). An incision is usually made behind the ear. The mastoid bone (a bone in the skull, behind the ear) is removed using high-speed drills, and any disease is eliminated from the mastoid. In traditional mastoid surgery, the ear canal is removed and a cavity created. Cavities often necessitate cleaning (one to four times per year by a physician), and many people with mastoid cavities cannot get water in them without causing infection. It is possible to do mastoid surgery leaving the ear canal intact. The ear drum is reconstructed and following such procedures, hearing can often be restored to normal, and people can shower, swim, and perform other activities without restriction.
- Translabyrinthine surgery (surgery through the inner ear) is performed to remove acoustic neuromas. This approach involves removal of the mastoid bone in order to enter the brain cavity. However, it always results in total loss of hearing. In most cases, the tumor has caused a significant hearing loss, and the roots of the tumor are embedded in the hearing nerve. This approach has many advantages, including minimizing trauma to the brain and preservation of the facial nerve, which lies near these tumors and is subject to swelling and temporary weakness. Occasionally some permanent weakness results.
- Middle Fossa and Retrosigmoid surgery removes smaller tumors and in some cases hearing may be preserved. The middle fossa approach goes above the ear and the retrosigmoid approach goes behind it. The risks are essentially the same as for translabyrinthine surgery in properly selected cases. As with translabyrinthine surgery, the facial nerve lies adjacent to the tumors and is subject to swelling and temporary weakness. Occasionally some permanent weakness results.
What Can I Do To Protect My Hearing?
Preventive medicine is always the best medicine. Here are some simple steps you can take to protect your hearing:
- Wear ear protectors when mowing the lawn or using a power saw.
- Pieces of cotton or paper towel (or spent bullet casings) stuffed in the ears are generally inadequate.
- With personal portable music systems, if the person standing next to you can tell what you are listening to through earphones, the music is probably too loud and should be turned down.
- Have your blood pressure checked regularly, and take medication to keep high blood pressure under control.
- Maintain healthy eating and exercise habits, and have regular physical exams.
- If you have a family history of hearing loss, you should have regular hearing tests so that problems can be recognized and addressed early.
Like so many other things, we rarely appreciate the value of hearing until it is lost. Through sensible preventive measures, many potential causes of hearing loss can be eliminated. When hearing loss occurs, its progression can sometimes be prevented or slowed. In every case, early diagnosis and treatment will minimize the psychological and social trauma so common in people with hearing impairment.
Hearing experts are constantly working to learn more about the conditions we don’t yet understand. Even for patients who can’t be cured today, there is always hope for tomorrow.
Hearing Loss: Frequently Asked Questions
Here are some frequently asked questions related to hearing loss.
Q: My daughter listens to loud music with headphones. Can this damage her hearing?
A: Loud music, especially listened to with earphones, can damage hearing. In some cases, the playing of musical instruments also can damage hearing. This has been reported not only with loud, electrical rock-and-roll instruments, but also with classical music performance such as violin playing and flute playing. One can minimize such problems by using ear protection whenever practical, such as during selected practice sessions. With personal portable music systems, if the person standing next to you can tell what you are listening to through earphones, the music is probably too loud.
Q: Lately, my grandfather has been saying “what?” almost every time someone speaks to him. Is this just a habit, or is it possible that he has some hearing loss?
A: Hearing loss can sneak up on people. Often family members and friends are aware of hearing problems before the hearing-impaired person. Many people in the early stages of hearing loss of this sort will find themselves asking “what?” more frequently. Other signs are offering inappropriate answers because they have misheard a conversation or question, or socializing less with others.
Q: Is it a good idea to remove wax inside the ear with cotton-tipped swabs?
A: No. The ear has a natural self-cleaning mechanism. Ear skin normally sheds from the inside out. If you place a drop of ink on the
Q: My son had a serious ear infection recently, and as a result his eardrum ruptured. Will he need surgery?
A: Most perforations (holes) in the eardrum heal spontaneously. When one does not, it can nearly always be repaired with surgery. The procedure is usually relatively fast, and may be performed under local anesthesia.
Q: Does family history play a role in hearing loss?
A: Family history is extremely important. Hearing loss is often hereditary. When it runs in families from generation to generation, the hearing loss usually follows a hereditary pattern called “autosomal dominant.” However, the absence of a family history does not mean that hearing loss is not genetic. “Autosomal recessive” inheritance is common. It means that neither parent has hearing loss, but both carry a gene that causes it. On the average, the hearing loss will be present in one child out of four.
Hearing Loss: Putting It All Together
Here is a summary of the important facts and information related to hearing loss.
- Hearing disorders are common. More than 40 million Americans have hearing loss.
- Good hearing is essential not only for communication and business, but also for many of the subtle joys that make life worth living.
- Hearing loss is often preventable and is nearly always treatable.
- Because hearing loss may be a symptom of a more serious underlying health problem, a medical checkup is important.
- Hearing loss can be reversed by treating underlying conditions or by performing surgery.
- Some people have their hearing ability restored with the help of hearing aids.
- There are simple steps you can take to help preserve your hearing.
Hearing Loss: Glossary
Here are definitions of medical terms related to hearing loss.
Acoustic nerve: The nerve that leads from the inner ear to the brain, serving as the pathway for the nerve impulses that the brain will interpret as sound; also called the eighth cranial or auditory nerve
Acoustic neuroma: A common tumor of the acoustic nerve (which serves as the pathway for hearing); it can cause hearing loss, can compress the brainstem and other nerves, and can usually be cured with surgery
Audiogram: A hearing test usually performed in a soundproof room; the person wears earphones and tones are presented to each ear, one at a time
Audiologist: A health professional with at least a master’s degree that studies the sense of hearing, detects and diagnoses hearing loss, and works to help individuals with hearing loss
Auditory canal: The channel in the ear
Cochlea: A hollow tube in the inner ear that is coiled to resemble a snail’s shell; it contains thin fluid and the organ of Corti, and it is where sound vibrations picked up by the middle ear are carried
Conductive hearing loss: Hearing loss due to any condition that interferes with the transmission of sound through the outer and middle ear to the inner ear; this type of hearing loss can be successfully treated in most cases
Eardrum: A thin membrane covered by skin that separates the outer ear from the middle ear; also called the tympanic membrane
Ear tubes: Small metal or plastic tubes inserted into the eardrum to ventilate the middle ear, or to allow the fluid from the middle ear to drain through the ear canal
Eustachian tube: The tube that connects the middle ear to the back of the throat; its function is to equalize the air pressure in the ear
Meniere’s syndrome: A condition characterized by fluctuating hearing loss (usually more prominent in the lower frequencies where we hear speech), dizziness, fluctuating ear pressure, and tinnitus (a noise sensation heard in one or both ears)
Myringotomy: A small incision made into the eardrum to allow fluid to drain from the ear
Organ of Corti: The part of the inner ear that contains thousands of hair-like cells; it functions as the switchboard of the hearing system by responding to different sound frequencies and converting them to nerve impulses
Ossicles: The chain of three small bones that connects the eardrum to the inner ear; the bones are the hammer (malleus), anvil (incus), and the stirrup (stapes)
Otolaryngologist: A physician who specializes in the diagnosis and treatment of diseases and injuries of the ears, nose, and throat
Otolaryngology: A branch of medicine dealing with the diagnosis and treatment of diseases and disorders of the ears, nose, and throat, and adjacent structures of the head and neck
Otology: The medical specialty of ear medicine and surgery; a sub-specialty of otolaryngology (ear, nose, and throat medicine)
Pinna: The trumpet-shaped outer part of the ear on each side of the head; also called the auricle
Sensorineural hearing loss: Hearing loss in which the damage lies in the inner ear, the acoustic nerve, or both; also called “nerve deafness”
Tinnitus: A noise sensation heard in one or both ears; it can be a sign of an underlying disorder but can occasionally occur for no apparent reason
Vestibular labyrinth: The portion of the inner ear that functions as part of the body’s balance mechanism
Hearing Loss: Additional Sources Of Information
Here are some reliable sources that can provide more information on hearing loss.
Sight & Hearing Association
Phone: 1-800-992-0424 or
Phone: 651-645-2546
http://www.sightandhearing.org
(a Minnesota-based nonprofit organization, founded in 1939 as the Minnesota Society for the Prevention of Blindness, that works to prevent the needless loss of vision and hearing)
Books
- Sataloff RT, Sataloff J. Hearing Loss, 3rd edition. Marcel Dekker, Inc., New York, NY, 1993.
- Sataloff RT, Sataloff J. Occupational Hearing Loss, 2nd edition, Marcel Dekker, Inc., New York, NY, 1993.