
In this Article
Angioplasty
What Is Coronary Angioplasty?
Coronary angioplasty is a medical procedure during which narrowed arteries that supply blood to the heart muscle are widened, to allow for improved flow of blood through these arteries to the heart, without the need for open heart surgery.
The purpose of angioplasty is to widen narrowed or blocked arteries, so that enough blood can get to the heart to deliver the oxygen it needs to function properly.
Angioplasty is designed to relieve the chest pain a person usually feels when the heart is not getting enough blood and oxygen. A successful angioplasty will improve symptoms such as chest pain and shortness of breath, and may improve survival in a limited number of individuals.


|
Nice To Know: Coronory is the latin word for ‘crown’. The arteries that supply the heart muscle with blood are known as the Arteries become narrowed by a build-up of fat and |


In an angioplasty:
- A specially trained doctor inserts a long, narrow tube (called a catheter) through a small cut in the thigh or the arm.
- The doctor threads the
catheter through blood vessels leading to the heart until it reaches the narrowed part of the artery. - The doctor positions a tiny balloon that is attached to the tip of the catheter right at site of the narrowing, and then inflates it with air. The pressure of the balloon flattens the plaque and allows the artery to open wider.
- Often, a tiny wire tube called a
stent is left inside the artery to hold it open.
Sometimes, instead of flattening open the plaque with a balloon, other angioplasty methods are used:
- Atherectomy is a form of angioplasty that uses tiny blades or a drill-like tip on the end of the catheter to cut away or drill through the plaque.
Laser angioplasty uses laser energy to destroy plaque.
About Coronary Heart Disease
Coronary artery disease (CAD) is the most common form of heart disease.
Coronary heart disease develops when one or more of the coronary arteries that supply the blood to the heart become narrower than they used to be, due to the buildup of cholesterol and other substances in the wall of the artery, affecting the blood flow to the heart muscle. Without an adequate blood supply, heart muscle tissue can be damaged.
Deposits of cholesterol and other fat-like substances can build up in the inner lining of these blood vessels and become coated with scar tissue, forming a cholesterol-rich bump in the blood vessel wall known asplaque. Plaque buildup narrows and hardens the blood vessel, a process called
Eventually these plaque deposits can build up to significantly reduce or block blood flow to the heart. A person may experience chest pain or discomfort from inadequate blood flow to the heart, especially during exercise when the heart needs more oxygen.
- Angina usually manifests as a feeling of pain, pressure, or tightness in the middle chest, especially behind the sternum (breastbone).
- The sensation may spread to the left shoulder, arm, and hand, or to the neck, throat, and jaw.
- The attack typically lasts for only a few minutes
An attack of angina does not cause permanent damage to the heart muscle. This is the main difference between angina and a heart attack, during which part of the heart muscle suffers permanent damage (unless the new clot-busting drugs are given in time).
|
Nice To Know: Angioplasty can be performed in arteries throughout the body. Angioplasty that is done in the arteries of the heart is called coronary angioplasty, while angioplasty that is done in arteries in other parts of the body is called peripheral angioplasty. |
|
Facts About Angioplasty
|
Why Is Angioplasty Done?
The two main reasons angioplasty is performed are for:
- Angina (chest pain) – A person may experience chest pain, or angina, during exercise or stress because the heart’s arteries are too narrow to carry enough blood and oxygen to meet the increased demand. Different types of angina are discussed below. In those suffering angina, who have not responded to standard medical treatments, and continue to have symptoms, angioplasty will be recommended.
- Heart attack – During a heart attack, an artery becomes completely blocked, cutting off blood and oxygen to part of the heart and causing that tissue to die. This is why heart attacks cause such severe pain. Reopening the artery right away can minimize the amount of heart tissue that is damaged during a heart attack. But this is not applicable for everyone after a heart attack.
Angioplasty will generally not be offered to people without symptoms (but who may have some blockage in a coronary artery), and angioplasty to a number of
Angina
Angina, or angina pectoris, is a medical term for chest pain that results from problems with the blood supply to the heart.
- The job of the heart is to pump oxygen-rich blood to the body and then return it to the lungs, where it picks up more oxygen.
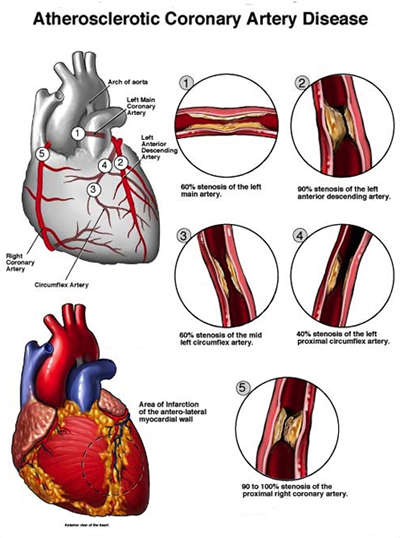
- The heart itself receives blood and oxygen through two major coronary arteries and the blood vessels that branch off of them. The most important of arteries supplying blood to the heart are the left main, left circumflex, left anterior descending, and right coronary arteries.
- Angina occurs when the coronary arteries are narrowed or blocked, and the heart muscle doesn’t receive enough blood and oxygen. This shortage of blood and oxygen causes pain in the chest.

The two main types of angina are:
- Stable angina – In stable angina, chest pain occurs during exercise or stress. How severe the pain is, and the kinds of situations that bring it on, are fairly predictable for each patient.
- Unstable angina – In unstable angina, chest pain is unpredictable and may come on suddenly, even during rest.
Stable Angina
Stable angina is caused by narrowing of the arteries of the heart. This results from
- People with stable angina may feel fine most of the time but experience chest pain when they climb a flight of stairs, do other types of exercise, or experience a stressful emotion, such as fear.
- Chest pain comes on during activity or stress because narrowed arteries may be able to supply only enough blood to the heart to keep up with less intense, everyday activities. Anything that causes the heart to beat faster and need more blood and oxygen can bring on chest pain.
- Stable angina may be treated with medications that reduce the stress on the heart or help the coronary arteries to open wider.
- If the medication doesn’t work well enough, or a person wants to lead a more active life, the doctor may recommend coronary angioplasty or
coronary artery bypass surgery . In bypass surgery, blood vessels are taken from another part of the body and sewn into place above and below the narrowing, creating a new route for blood to travel that bypasses the trouble spot.
Unstable Angina
This type of angina, which causes a temporary, often-severe feeling of chest pain or pressure, is a more serious condition and requires immediate treatment. Unstable angina can indicate the artery is becoming increasingly narrowed and is in danger of becoming blocked completely, or that a blood clot may be forming, causing off-and-on blockage of the artery. These conditions can cause a heart attack.
- Unstable
angina usually is treated with medications that reduce the blood’s ability to clot. During treatment, patients are observed closely in the hospital to make sure they don’t develop a heart attack. - If medication isn’t effective and the heart continues to receive too little blood and oxygen, angioplasty or coronary artery bypass surgery may be required.
|
Nice To Know: What is variant angina? A third type of angina, known as ‘variant angina’, is caused by a spasm of the coronary artery, and usually doesn’t damage the heart or require angioplasty or surgery. |
For further information about angina and its treatment, go to Angina.
Heart Attack
Angioplasty is also performed as an emergency procedure to widen the coronary arteries of a patient who is suffering, or who has just suffered, a heart attack.
- A heart attack is caused by a completely blocked coronary artery. Usually an artery becomes blocked when a section of soft, inflamed plaque breaks open at one end, causing a blood clot to grow and fill the inside of the artery. When this happens, no blood can get to the part of the heart that had been supplied by the blocked artery.
- In the past, heart attack treatment with angioplasty or clot-dissolving medication were viewed as equally good choices.
- Now angioplasty is seen as the preferred treatment, because it can open the blocked coronary artery faster than clot-dissolving drugs can.
- The disadvantage of angioplasty for the treatment of heart attack is that it is not available in many U.S. hospitals. To do angioplasty safely and well during a heart attack, hospitals must have the necessary equipment and a team of experienced cardiologists, nurses, and technicians ready at a moment’s notice, 24 hours a day. Generally, only very large medical centers have this type of program in place.
For further information about heart attack and its treatment, go to Heart Attack.

|
Nice To Know: My doctor says I have coronary artery disease that requires surgical treatment. I would like to have an angioplasty, but my doctor says it won’t work for me. Why not? Not all plaques respond to the angioplasty technique; some are too long or too hardened, or out of reach of the |
|
Nice To Know: Finding hidden coronary artery disease Some people may also have angioplasty without ever having experienced chest pain. Usually these are people who:
As a precaution, they may have an exercise stress test or some other type of screening exam. If the results lead the doctor to suspect heart disease, the person may have a diagnostic test called an angiogram, or cardiac catheterization. This is an x-ray of the arteries that involves injection of a special x-ray dye that helps to show whether there are severe narrowings in the coronary arteries. If there are, the doctor may recommend angioplasty or bypass surgery. |
Different Types Of Angioplasty
The purpose of angioplasty is to widen the coronary arteries of the heart that have been narrowed or completely blocked by plaque build-up or a blood clot. Specifically which angioplasty technique the cardiologist uses depends on where the narrowing is, how it is shaped, and whether it is made of hard or soft plaque.
The cardiologist can choose from the following options:
These procedures are all variations on the original form of balloon angioplasty. They differ mainly in the type of instruments used.
Balloon Angioplasty
Balloon angioplasty is performed by passing a thin tube, or

Laser Angioplasty
Laser angioplasty is similar to balloon angioplasty, but instead of a balloon-tipped catheter, one with a laser at the tip is used. The laser is guided to the blockage, then used to destroy the plaque, layer by layer, by vaporizing it into gaseous particles.
The laser can be used alone, or in combination with balloon angioplasty. If it is teamed up with balloon angioplasty, with the balloon inserted first to attack the hard plaque. The first laser device (the “excimer laser”) for opening coronary arteries won U.S. governmental approval in 1992 but is not used as frequently as other angioplasty procedures.
Coronary Atherectomy
This procedure is begun similar to angioplasty. But instead of a balloon pressing against the fatty deposits in the walls of the arteries, special instruments are used which cut away the plaque.
This technique is proving very useful in treating blockages that may be too calcified (hardened) or inaccessible for balloon angioplasty. The devices that can be used are:
- Extraction atherectomy – This procedure uses a tiny rotating blade that works in much the same fashion as the cutter on a food processor to whisk away blockages inside the artery wall at a rate of up to 1,200 revolutions per minute.
- Rotational atherectomy – This procedure uses a high-speed, diamond-tipped drill to penetrate fatty deposits and is particularly useful on hard, calcified plaque.
- Directional atherectomy – This procedure uses a device that is a combination of a balloon and a shaving blade. The cutting device, usually located on the side, is run back and forth and shaves the deposits away.
Coronary Stenting
Stents are small, expandable, metal devices inserted by a catheter into a narrowed artery after the angioplasty procedure is complete. Stents are left in place to help keep the artery from closing again (a complication called
- Since the first coronary
stent was approved in 1993, these devices have gained widespread acceptance. - Stents are now used in combination with balloon angioplasty an estimated 60% to 70% of the time. Direct coronary stenting, which is done without balloon angioplasty, is also an option, but is not used as frequently.
- Generally, stents have improved the outcome of patients who have angioplasty. On rare occasions, a patient can develop blood clots associated with the use of stents. This occurs more often in people with weak hearts, and after the use of more than one stent, or different types of stents.
|
Nice To Know: Drilling channels in the heart: When neither angioplasty or bypass surgery is an option Laser revascularization, also called transmyocardial revascularization (TMR), is an experimental procedure that is being studied as a way to relieve severe TMR is sometimes called the “snake heart” procedure, because the surgeon duplicates the design of the reptile heart by using a laser to create open channels in the heart muscle. The goal is to enable the lower chamber of the heart, called the ventricle, to pump blood directly through the newly created channels into the heart muscle, rather than relying on blood vessels to do the job. This procedure has produced early promising results in relieving chest pain, but no long-term studies have been done. Researchers still have many questions about whether it really benefits patients. |
Preparing For An Angioplasty
After scheduling angioplasty, the cardiologist or another member of the medical team will review all the details about the angioplasty procedure, including:
- The diagnostic cardiac catheterization that will be performed beforehand
- What to do the night and morning before the procedure
- What happens during the procedure
- What happens during recovery
- What to do after arriving home
Cardiac Catheterization
Before angioplasty, patients usually have a diagnostic test called
In this procedure:
- A
catheter is threaded through the blood vessels leading to the heart - A special contrast dye that shows up on x-rays is injected into the
coronary arteries - X-ray images are taken to look for narrowed areas in the arteries and determine how severe the narrowings are.
In addition to being used to definitively diagnose
Usually, the catheterization is done first, with the patient returning at a later time for the angioplasty. If the test results show that an artery is dangerously narrowed, angioplasty may be performed immediately.
Getting Ready For Angioplasty
It is important to follow a few simple precautions before angioplasty. Talk to the doctor about how to prepare for the procedure.
- Do not eat or drink anything after midnight the night before.
- Ask the doctor about taking regular medications the morning of the angioplasty.
The Procedure
Coronary angioplasty is performed in a cardiac catheterization laboratory, generally by an interventional cardiologist, who has received special training and certification in the procedure.
- Before the procedure, patients are given a sedative to help them relax.
- An intravenous line is started in a vein in the arm, so that fluids and medications can be easily given during the procedure.
- A local anesthetic is injected in the skin near the femoral artery, the artery that leads from the groin to the coronary arteries. (Sometimes, the artery in an arm, the brachial artery, is used instead).
- To start the angioplasty procedure, the interventional cardiologist makes an incision and inserts a thin, hollow catheter through the artery, threading it up toward the heart and into the coronary artery that contains the blockage. X-ray photography enables the cardiologist to view the movement of the catheter on a TV monitor.
- After the catheter arrives at the site of the blockage, a second, thinner catheter is inserted into the first one. There is a small, deflated balloon at the tip of the second catheter.
- Once the balloon is in position at the site of the narrowing, it is inflated. The temporary widening of the artery either crushes or breaks the
plaque , and the balloon is then removed. The artery is widened by the balloon inflation, and blood flow improves. - The balloon may be reinflated one or two times to keep the artery open. If a coronary
stent is used, a new catheter is inserted to guide the stent into place. Once in place, the stent pushes against the wall of the artery to keep it open. - The procedure usually takes about two hours, depending on the number and severity of the blockages.
What Happens Afterward?
Sedatives take a while to wear off, so many patients sleep after the procedure. After the catheter is removed, the cardiologist or another hospital worker will apply heavy pressure to the incision in the groin or arm for about 20 minutes to stop any bleeding, while the patient lies in bed, remaining still.
- In some hospitals, a special device is used to apply pressure, rather than a person.
- It is important to stay in bed for about six hours after angioplasty. Later, a nurse or medical technician will assist the patient in getting out of bed and walking around.
- The patient usually stays in the hospital overnight. If no problems such as bleeding or chest pain occur, the patient usually goes home the following day.
- A family member or friend should drive the patient home.
After Arriving Home
After angioplasty, it’s a good idea to relax and take it easy for a few days.
- Avoid driving a car with a standard transmission for a few days to rest the leg where the catheter was inserted.
- It is safe to return to a desk job almost immediately. However, your doctor may advise waiting for several days before returning to a job that involves using the legs a lot or bending or lifting.
- Many patients take some type of blood-thinning drug to prevent blood clots angioplasty. Talk to the doctor about exactly how to take the drug.
- The cardiologist will probably schedule a return visit at six weeks for an exercise stress test or other form of stress test. This is done to make sure that the arteries have remained open, and also to furnish results that can be used for comparative purposes if chest pain or other symptoms develop later on.
- If chest pain or other cardiac symptoms return, contact the doctor immediately.
Risks And Possible Complications of Angioplasty
Angioplasty is considered safe and effective, although, as with all medical treatments, there is some risk. In general, possible complications fall into two categories:
- Acute complications – These are complications that occasionally occur during the procedure or immediately afterward.
- Long-term complications – Even when the angioplasty procedure is performed without problems, the artery can narrow again months afterward, causing chest pain to return. This complication is called restenosis.
Acute Complications
Angioplasty is a very safe procedure when performed by experienced cardiologists at top-notch medical centers. In a small percentage of patients, an artery may abruptly close during the procedure, which may trigger a heart attack. A heart attack may also occur if a blood clot is dislodged during angioplasty and completely blocks the artery, cutting off blood and oxygen to the heart.
These complications may or may not require emergency bypass surgery. The death rate among patients who have angioplasty is very tiny, about 0.1% (compared to 1% to 2% for routine bypass surgery).
Restenosis
Restenosis is the most troublesome problem hampering the success of angioplasty. Restenosis is a medical term that refers to the gradual re-narrowing of the artery during several months following the procedure.
- Sometimes, restenosis is caused by blood clots occurring at or near the site of the treatment. Aspirin, heparin, or combinations of anti-clotting drugs are generally used before and after the procedures to try and prevent this.
- Coronary stents that are coated with anti-clotting drugs are now being used in the hope of preventing the immediate formation of blood clots and, over time, restenosis.
Researchers are gaining a better understanding of the restenosis process and experimenting with several different approaches to prevent it. They believe that three complex, interrelated mechanisms are involved.
- Within hours after an angioplasty procedure, the walls of the artery may start to recoil, gradually “caving in” to their original position. This can reduce the channel that was created, sometimes by as much as half.
- Angioplasty, by pressing against the artery wall and creating tiny cracks in the
plaque , causes a certain amount of injury to the artery wall. As the body attempts to heal itself, special blood cells that are involved in clotting, called platelets, may accumulate, possibly causing a blood clot. - Blood clots create a substance, thrombin, that causes the cells of the artery to multiply and new tissue to form. This is a helpful part of the healing process – but, if too much tissue is formed, it can reduce the flow of blood through the artery.
Thanks to an improved understanding of restenosis, several drugs are now being tested to help prevent it.
The reason restenosis occurs is not known, but several conditions increase the risk that the artery will narrow again after angioplasty. These include:
- High blood pressure
- Diabetes
Angina , both unstable and stable- Kidney disease requiring dialysis
There is also a theory that procedures affecting blood vessels activate cytomegalovirus (CMV), a herpes virus that is common in older people but is usually dormant. According to this theory, CMV is the factor that allows too many cells to multiply during the artery’s healing process and eventually narrows the artery again.
|
Nice To Know: Q: I had an angioplasty performed and I’m concerned about the vessel reclosing. How do I know whether or not this is happening? A: Usually, the return of chest pain (angina) is the chief symptom of reclosure, or restenosis. About 60% to 70% of patients who develop restenosis will experience chest pain. Contact your doctor if you begin suffering chest pain. However, not everyone who develops restenosis experiences chest pain, which is why you should contact your doctor if you experience unusual fatigue, shortness of breath, chest pressure, or any of the other symptoms you may have had before your angioplasty. About 10% to 20% of patients who develop restenosis experience no symptoms at all. |
What Are The Advantages Of Angioplasty Over Bypass Surgery?
A person who has been taking medication for angina but is still experiencing frequent or severe chest pain may need either angioplasty to widen the narrowed artery, or coronary artery bypass surgery to create a different blood vessel for supplying the heart with blood.
Over the long run, the two procedures are equally successful in getting rid of chest pain and in preventing a heart attack or death. Angioplasty is an easier procedure to go through, however.
Some of its advantages are:
- Recovery is much shorter and less painful, requiring a one- or two-day hospital stay, compared to a stay for a week or more for bypass surgery. Some hospitals are now performing angioplasty on low-risk patients in the morning and sending them home the same day.
- Angioplasty can be performed under local anesthesia (where the patient is sedated but awake), as opposed to general anesthesia (where the patient is asleep), which is needed for bypass surgery. There are more risks associated with general anesthesia, although those risks are small.
- The chest does not need to be opened, an advantage that substantially reduces pain, recovery time, and scarring.
- There is no need to use a heart-lung machine; this type of machine makes bypass surgery easier to do but increases the possibility of stroke.
However, some angioplasty patients must have the procedure repeated within a few months, because the artery may become narrowed once again, a problem that is called
In angoplasty procedures today, stents often are used to keep an artery open after it is widened, which helps reduce the risk of restenosis.
|
Nice To Know: Q: My doctor recommends I have an angioplasty, but also warns me that they sometimes need to be redone over the next several months. So wouldn’t it make more sense to have coronary bypass surgery instead? A: Because angioplasty restores blood flow to the heart without the need for major surgery, most doctors are inclined to try it at least once, unless there are clear indications it is unsuitable. Even if a repeat angioplasty is needed to achieve lasting results, this is still less stressful on the body than coronary bypass surgery. |
For further information about cardiac bypass surgery, go to Cardiac Bypass Surgery.
Who Does Angioplasty Benefit?
As techniques and equipment improve, angioplasty is being done successfully in a wider and wider range of individuals. Generally, however, angioplasty is an option for patients who have the following:
- Angina pain that cannot be controlled by medication
- Severe narrowing of one or more arteries that poses a significant threat to a large area of heart muscle
- Severe narrowing of the left anterior descending artery (which supplies blood to a large part of the heart), but only if the heart muscle has not been significantly weakened by previous damage
Who Does Angioplasty Not Benefit?
Angioplasty is safe and effective, but it is not the right procedure for everyone with angina. Some narrowings can’t be treated effectively or safely with angioplasty.
For example, some people may have severe
The cardiologist may decide against performing
- Severe narrowing of the left main coronary artery (because this major artery branches into several others, putting too much of the heart at risk if the angioplasty were to fail)
- Severe narrowing of any three arteries in a person who also has a weakly pumping heart
- Severe narrowing of the left anterior descending artery and at least one other coronary artery, plus either diabetes or a weakly pumping heart
|
Need To Know: Angioplasty and Diabetes Major studies have recently suggested that people who have diabetes in addition to |
|
Nice To Know: Q: My doctor says I have coronary artery disease that requires surgical treatment. I would like to have an angioplasty, but my doctor says it won’t work for me. Why not? A: Not all plaques respond to the angioplasty technique; some are too long or too hardened, or out of reach of the |
|
Nice To Know: A little heart math One way a cardiologist judges whether a patient should have angioplasty or bypass surgery is to measure whether the heart is pumping strongly or weakly. This is especially true when the artery that needs to be widened supplies a large section of the heart. To make this measurement takes a little math. Using one of several possible imaging methods, the cardiologist measures:
Generally, a heart that can squeeze out at least half of the blood that fills the ventricle with each heartbeat. That is, a heart that has an ejection fraction of 50% or more is considered to be pumping strongly enough to withstand angioplasty of a major artery, such as the left anterior descending artery. |
Frequently Asked Questions: Angioplasty
Here are some frequently asked questions related to angioplasty.
Q: My doctor has told me I should have an angioplasty. How do I choose who should do it and where it should be done?
A: As with other medical procedures, practice makes perfect, and the volume of procedures done, both by the physician and the hospital where the procedure is performed, is important. According to joint guidelines set by the American Heart Association and the American College of Cardiology, the hospital itself should be the site of at least 200 angioplasties each year, so that the entire angioplasty team becomes expert in doing angioplasty.
Q: My doctor recommends I have an angioplasty, but also warns me that they sometimes need to be redone over the next several months. So wouldn’t it make more sense to have coronary bypass surgery instead?
A: Because angioplasty restores blood flow to the heart without the need for major surgery, most doctors are inclined to try it at least once, unless there are clear indications it is unsuitable. Even if a repeat angioplasty is needed to achieve lasting results, this is still less stressful on the body than coronary bypass surgery.
Q: I had angioplasty, but my doctor still recommends that I lower my
A: An angioplasty treats the result of
Q: My doctor says I have coronary artery disease that requires surgical treatment. I would like to have an angioplasty, but my doctor says it won’t work for me. Why not?
A: Not all plaques respond to the angioplasty technique; some are too long or too hardened, or out of reach of the
Q: I had an angioplasty performed and I’m concerned about the vessel reclosing. How do I know whether or not this is happening?
A: Usually, the return of chest pain (angina) is the chief symptom of reclosure, or
Q: I am a diabetic. Should I have an angioplasty?
A: Major studies have found that the death, complication, and restenosis rates for diabetics who have angioplasty is significantly higher than for those who have coronary bypass surgery. This doesn’t necessarily rule angioplasty out. It may still be the best procedure for you. Your doctor will take your diabetes into consideration, along with other factors, to determine the best treatment.
Putting It All Together: Angioplasty
Here is a summary of the important facts and information related to angioplasty.
- Angioplasty is now the most common procedure performed to widen
coronary arteries narrowed bycoronary artery disease . - Angioplasty can be done using one of several instruments attached to the end of a long, thin tube, called a
catheter . These instruments include a balloon, a laser, and a drill. Often, they can be used together. Currently, the most popular approach isballoon angioplasty in combination with coronary stenting. - The popularity of angioplasty is due to its ability to increase the flow of blood through the coronary arteries without the need for major surgery.
- The situations in which angioplasty is used has broadened considerably over the years, from simple blockages in just one artery to more complicated cases involving several arteries. Still, angioplasty is not appropriate for everyone.
- Angioplasty was once a two-day procedure, but now patients go home much sooner, usually the next day. Some hospitals are even doing angioplasty on an outpatient basis (without an overnight hospital stay) for patients who are otherwise healthy and whose procedures are uncomplicated.
- The most common complication of angioplasty is
restenosis , or reclosure of the artery widened by angioplasty.
Glossary: Angioplasty
Here are definitions of medical terms related to angioplasty.
Angina: Temporary chest pain or feeling of pressure that occurs because the heart is not getting enough oxygen due to the diminished blood flow to the heart. There are two types: stable and unstable.
Angioplasty: A procedure in which a physician threads a catheter through blood vessels and uses a balloon or other device attached to the tip of the catheter to widen the arteries that have been narrowed by artery disease.
Atherosclerosis: A disease of arteries, including the arteries of the heart in which the inner layers of the artery walls become thick and irregular due to deposits of fat, cholesterol, and other substances.
Balloon Angioplasty: A procedure in which a balloon-tipped catheter is used to widen a narrowed artery.
Catheter: A thin tube that is threaded through the blood vessels.
Cholesterol: A fat-like material that is eaten as part of meat and other animal products, and is also made by the human body. Cholesterol has several beneficial uses in the body, but it can also be harmful when it builds up in the walls of arteries and causes them to narrow.
Coronary angiography: An x-ray procedure in which a catheter is threaded through the blood vessels leading to the heart and special x-ray dye is injected. It enabling the cardiologist to see whether the arteries in the heart are narrowed or blocked by plaque build-up or a blood clot and how severe the problem is.
Coronary arteries: The arteries that provide blood to the heart muscle. The most important of the arteries supplying blood to the heart are the left main, left circumflex, left anterior descending, and right coronary arteries.
Coronary artery bypass surgery: Also known as coronary artery bypass grafting (CABG-pronounced CABBAGE), this surgery involves taking a portion of a blood vessel from another part of the body, usually the leg or chest, and surgically attaching it across a severely narrowed or blocked coronary artery, thus ‘bypassing’ the blockage to improve blood supply to the heart muscle.
Coronary artery disease: The narrowing of the coronary arteries of the heart caused by deposits of cholesterol, fat, and other substances that form plaque.
Coronary atherectomy: Removing the blockage within the coronary artery, by using a cutting device to shave, cut, or drill through the blockage in the artery in order to widen it.
Interventional cardiology: A subspecialty of cardiology that uses catheters and other devices to restore blood flow to the heart without the need for major surgery.
Laser angioplasty: A procedure in which a laser-tipped catheter is used to widen a blocked artery.
Plaque: The deposits of fat, cholesterol, and other substances within the walls of an artery causing the artery to become narrowed.
Restenosis: The gradual reclosing of an artery after it has been widened.
Revascularization Procedure: A broad term that describes any procedure that is used to restore blood flow to the heart.
Stent: A small, metal or plastic device inserted by a catheter into a narrowed artery wall and then left in place, to help keep the artery open.
Additional Sources Of Information: Angioplasty
Here are some reliable sources that can provide more information on angioplasty.
American College of Cardiology Heart House
Phone: 301-897-5400
Phone: 800-253-4636
American Heart Association
Phone: 800-227-2345
Phone: 214-373-6300
National Heart, Lung and Blood Institute (NHLBI) Information Center
Phone: 800-575-WELL
Phone: 301-251-1222