
In this Article
Melanoma
What Is Melanoma?
Melanoma is a rare but potentially serious type of skin cancer.
Skin cancer is a disease in which skin cells lose the ability to divide and grow normally. These abnormal skin cells can grow and form a mass or “tumor.”
A skin tumor is considered benign (not cancer) if it is limited to a few cell layers and does not invade surrounding tissues or organs. If the tumor spreads to surrounding tissues, it is considered malignant, or cancerous. Cancer cells crowd out and destroy nearby healthy cells, forming growths called malignant tumors.
Most skin growths are benign tumors. However, melanoma is a malignant skin growth because it can
Malignant melanoma has a very high cure rate if diagnosed early and treated promptly.
Melanoma that spreads to vital organs like the brain or liver can be life-threatening.
Understanding how melanoma develops:
The skin is made up of 3 layers:
- The
epidermis , or outer layer of skin, which is made up of three different types of cells - The
dermis , or middle layer of the skin; it contains nerves, blood vessels, sweat glands, hair follicles, and oil-producing cells that keep the skin from drying out - The fatty layer

The epidermis in made up of 3 different types of cells. Different types of skin cancer are named for the kind of cell that becomes malignant.
Basal cell carcinoma starts in basal cells, which are small, round cells found at the base of the epidermis. It is the most common kind of skin cancer. More than 90 percent of all skin cancers in the United States are basal cell carcinomas. Basal cell carcinoma is the least serious kind of skin cancer because it grows slowly and seldom spreads.Squamous cell carcinoma starts in squamous cells, which are flat scaly cells that form the outermost part of the skin. Squamous cell carcinoma is more serious because it spreads more often than basal cell carcinoma. However, squamous cell carcinoma usually spreads slowly.- Melanoma starts in the
melanocytes , which are pigment-producing cells found mainly in the lower part of the epidermis (the outer layer of the skin). They make a dark material, melanin, which gives skin its natural color. Melanoma is serious because the malignant cells tend to spread rapidly from the skin to internal organs.
|
Melanomas may form from an existing mole or freckle, or begin to grow from a normal-appearing area of the skin. |
|
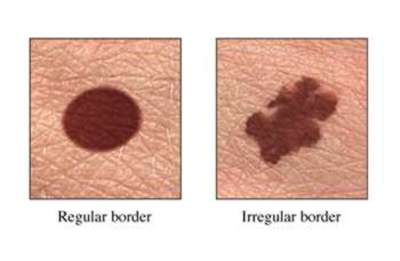
Melanomas vs. normal moles:
|
|
Melanomas often show the ABCD symptoms:
|
|
If a mole changes size or appearance, or bleeds, or becomes a wound that does not heal then you must have this looked at by a doctor as it may be a sign of cancer. |
|
Your chances of finding skin cancer can be improved by performing a regular skin examination at home. Follow these tips:
By checking your skin regularly, you will become familiar with what is normal. If you find anything unusual, see your doctor right away. Remember, the earlier skin cancer is found, the better the chance for cure. The following self-exam routine should take no more than 15 minutes:
|
|
Nice To Know: Q. My mother had melanoma. I’m worried that I may get it, too, especially because I have a lot of moles on my skin. What kind of medical checkups are recommended? A. Melanoma does run in families. If your parents had melanoma, your own risk may be higher than normal – especially if you have many moles of a certain kind. Your primary care doctor should do a total skin examination at each routine physical examination. That involves inspecting every inch of your skin, including the genital region and the area between the buttocks. If the doctor spots suspicious growths, you’ll probably get a referral to a |
Although most pigment-producing cells are in the skin, some of these types of cells occur in other parts of the body and can also become malignant. For example,
|
Facts About Melanoma
|
Who is most at risk of developing melanoma?
Anyone can get melanoma. Certain individuals, however, have several risk factors for melanoma. They are at higher risk for getting the disease than the general population. But risk factors do not cause a disease. Many people with risk factors for melanoma never get the condition.
People with higher-than-normal risk include those who have or have had:
- Many moles: Individuals who have certain types of moles, typically bigger than ordinary moles (also called ‘dysplastic nevi’), are at a greater risk of developing
malignant melanoma. To learn more about moles see What are moles? - Family history of melanoma: Having parents or siblings who have had malignant melanoma increases a person’s risk. A person with dysplastic nevi and at least two close relatives with melanoma has a 50 percent higher risk of developing melanoma.
- Personal history of melanoma: A person who has had melanoma before may get it again in a different part of the skin. Melanoma that was treated also may
recur . - Sun exposure: People who work or spend lots of leisure time outside are at increased risk for all skin cancers. People who live at higher elevations are also at greater risk because the atmosphere is thinner and does not filter UV rays as well.
- Sunburn: Having one or more blistering sunburns before the age of 20 increases risk for developing melanoma later in life. Severe sunburns in adults also increase risk.
- Immune suppression drugs: The body’s immune system detects and destroys cancer cells. Immune suppression drugs may weaken this protective action. Drugs used to prevent rejection of transplanted organs and treat cancer are among those that suppress the immune system.
- Advanced age: Almost half of all melanoma cases are diagnosed in individuals age 50 and over. Yet melanoma is also one of the most common cancers diagnosed in people under 35.
What Is Your Personal Risk?
Use this skin type table to determine your susceptibility to skin cancer:
|
SKIN TYPE(Fitzpatrick) |
*RESPONSE TO SUN EXPOSURE |
EXAMPLES |
SUSCEPTIBILITY |
|
I |
Always sunburn, don’t tan |
Fair-skinned & freckled |
Very High |
|
II |
Always sunburn tan minimally |
Fair-skinned, blonde haired, Blue-eyed, Scandinavians |
High |
|
III |
Sometimes sunburn, tan moderately |
Fair-skinned, brown hair, brown-eyed; unexposed skin is white |
Average |
|
IV |
Seldom sunburn, tan easily |
Light brown skin, dark brown hair, brown-eyed; unexposed skin is tan; Mediterranean, Hispanic |
Low |
|
V |
Rarely sunburn, tan profusely |
Dark brown skin; Mediterranean, Asian, Eastern Indian |
Very low |
|
VI |
Never sunburn, Deeply pigmented |
Black |
Minimal |
* Generally based on first exposure to sun following a long period without exposure
Moles
What are Moles
Moles are small, usually dark skin growths composed of a group of cells called melanocytes. These cells make the pigment melanin. Moles are very common. The average adult has about 40 to 60 moles and other skin growths.
Moles often are black, brown, or tan. They usually are no bigger than a pencil eraser and are round or oval in shape. Moles may be flat or raised. They may be present at birth or develop during childhood, and almost all are present by age 40.
The medical name for a
Certain kinds of moles called dysplastic nevi, or atypical moles, are typically bigger than ordinary moles. They look different than regular moles. They may appear on sun-exposed areas of the skin, or on areas that get little sunlight, like the buttocks or scalp. Dysplastic nevi tend to run in families. Individuals who have dysplastic nevi are at a greater risk of developing malignant melanoma, especially if they have a positive family history of melanoma.
The average person has dozens of moles and other benign skin growths. They include:
- Birthmarks, or “nevi,” are moles that are present at birth.
- Acquired moles begin to develop early in adolescence, growing and darkening throughout the teenage years. Many adults have 40 to 60 acquired moles.
- Liver spots, or “solar lentigines,” are flat tan-to-brown spots that occur mainly on the face, neck, hands, and forearms. They have nothing to do with the liver. Rather, they develop as a result of aging and sun exposure.
- Seborrheic keratoses are raised, wart-like, tan-to-brown growths that occur as people age.
- Acquired cherry angiomas are smooth, dome-shaped red spots that usually develop on the chest and back. Most are bright red and appear as people age.
- Skin tags are small, soft flaps of skin that grow on the neck, in the armpits, and groin area.
- Actinic keratoses are slightly scaly, reddish patches that form on people with sun-damaged skin. They are pre-cancerous growths that may change into a squamous cell carcinoma, so doctors usually recommend having them removed.
Although most skin growths are not cancer, it’s important to check with the doctor about new growths or changes in old growths.
In many cases, the first sign of skin cancer is a mole that changes in size or color, or becomes a sore that does not heal.
What Causes Melanoma?
Experts believe that many cases of melanoma are caused by excessive exposure to ultraviolet (UV) radiation from the sun. Energy from the sun is a form of radiation. It consists of visible light and other rays that people can’t see. Invisible infrared radiation, for instance, makes sunlight feel hot. UV also is invisible, and causes sunburn and suntan.
UV rays damage DNA, the genetic material that makes up genes. Genes control the growth and health of skin cells. If the genetic damage is severe, a normal skin cell may begin to grow in the uncontrolled, disorderly way of cancer cells. UV rays also cause sunburn and other damage that makes the skin wrinkle prematurely.
There are two kinds of rays in ultraviolet radiation:
- ultraviolet A (UVA)
- ultraviolet B (UVB)
Scientists once thought that UVA rays were the main cause of melanoma. Now they think that UVB rays are also involved. That’s why it is important to use a
Abnormal genes that children inherit from their parents may make them more likely to get melanoma. Inherited genetic characteristics can include physical appearance (such as pale skin) as well as hidden tendencies to develop certain diseases. Scientists have discovered a gene, called the p16 gene, than can cause
|
Need to Know: People with close relatives who had malignant melanoma may have inherited a damaged gene that increases their risk for skin cancer. For them, preventive measures and regular skin exams can be especially important. |
Melanoma: Who Is Most At Risk?
Anyone can get melanoma. Certain individuals, however, have several risk factors for melanoma. They are at higher risk for getting the disease than the general population. But risk factors do not cause a disease. Many people with risk factors for melanoma never get the condition.
People with higher-than-normal risk include those who have or have had:
- Many moles: Individuals who have certain types of moles, typically bigger than ordinary moles (also called ‘dysplastic nevi’), are at a greater risk of developing
malignant melanoma. - Family history of melanoma: Having parents or siblings who have had malignant melanoma increases a person’s risk. A person with dysplastic nevi and at least two close relatives with melanoma has a 50 percent higher risk of developing melanoma.
- Personal history of melanoma: A person who has had melanoma before may get it again in a different part of the skin. Melanoma that was treated also may
recur . - Sun exposure: People who work or spend lots of leisure time outside are at increased risk for all skin cancers. People who live at higher elevations are also at greater risk because the atmosphere is thinner and does not filter UV rays as well.
- Sunburn: Having one or more blistering sunburns before the age of 20 increases risk for developing melanoma later in life. Severe sunburns in adults also increase risk.
- Immune suppression drugs: The body’s immune system detects and destroys cancer cells. Immune suppression drugs may weaken this protective action. Drugs used to prevent rejection of transplanted organs and treat cancer are among those that suppress the immune system.
- Advanced age: Almost half of all melanoma cases are diagnosed in individuals age 50 and over. Yet melanoma is also one of the most common cancers diagnosed in people under 35.
What Is Your Personal Risk?
Use this skin type table to determine your susceptibility to skin cancer:
|
SKIN TYPE(Fitzpatrick) |
*RESPONSE TO SUN EXPOSURE |
EXAMPLES |
SUSCEPTIBILITY |
|
I |
Always sunburn, don’t tan |
Fair-skinned & freckled |
Very High |
|
II |
Always sunburn tan minimally |
Fair-skinned, blonde haired, Blue-eyed, Scandinavians |
High |
|
III |
Sometimes sunburn, tan moderately |
Fair-skinned, brown hair, brown-eyed; unexposed skin is white |
Average |
|
IV |
Seldom sunburn, tan easily |
Light brown skin, dark brown hair, brown-eyed; unexposed skin is tan; Mediterranean, Hispanic |
Low |
|
V |
Rarely sunburn, tan profusely |
Dark brown skin; Mediterranean, Asian, Eastern Indian |
Very low |
|
VI |
Never sunburn, Deeply pigmented |
Black |
Minimal |
* Generally based on first exposure to sun following a long period without exposure
What Are The Symptoms Of Melanoma?
Melanoma is often painless and usually produces the following signs:
- A change in the size, color, shape, or feel of an existing mole
- The appearance of a new growth or mole on the skin
|
Need To Know: What changes in moles or freckles can indicate cancer? Melanomas may form from an existing mole or freckle, or begin to grow from a normal-appearing area of the skin. Any change in a mole’s appearance or the growth of a new mole may be a sign of skin cancer. Suspicious moles or freckles should be checked by a doctor. Melanomas vs. normal moles:
Melanomas often show the ABCD symptoms:
Watch for the ABCD signs when doing skin self-examination. Regular skin self-examination allows individuals to keep watch on moles and other skin growths. When existing growths change or new growths appear, check with the doctor. Like other forms of cancer, melanoma is most curable when diagnosed and treated early. |
|
Nice To Know: Q. My mother had melanoma. I’m worried that I may get it, too, especially because I have a lot of moles on my skin. What kind of medical checkups are recommended? A. Melanoma does run in families. If your parents had melanoma, your own risk may be higher than normal – especially if you have many moles of a certain kind. Your primary care doctor should do a total skin examination at each routine physical examination. That involves inspecting every inch of your skin, including the genital region and the area between the buttocks. If the doctor spots suspicious growths, you’ll probably get a referral to a |
How Is Melanoma Diagnosed?
Doctors often spot melanoma during a skin inspection. The doctor should look for growths by doing a complete examination of the entire skin surface during each yearly physical examination.
Many people detect melanoma themselves while doing regular skin self-examination. Early diagnosis is important-skin cancer would be almost 100 percent curable if all skin cancers were found and treated early.
|
Need To Know: Regular skin self-examinations and examinations by the doctor are especially important for people who have a higher-than-normal risk for melanoma. |
A
The type of biopsy depends on the size of the skin growth and its location on the body. Several types of biopsy can be done when the doctor suspects melanoma:
- An excisional biopsy excises, or cuts away, the entire growth with a margin of normal surrounding skin. The skin may be stitched together to close the hole. This procedure is more time-consuming and therefore usually needs to be scheduled. Generally, an additional wide local excision of normal surrounding skin will be required if the biopsy is positive. The width of the margin will depend on the thickness of the cancer.
- An incisional biopsy, or core biopsy, removes only a sample of the growth, and the resulting hole is closed with stitches. Further treatment is necessary if the microscopic examination reveals cancer cells.
- A punch biopsy removes a small, cylindrical shaped sample of skin. It includes the
epidermis ,dermis , and parts of the underlying tissue. It is done with a surgical tool that looks like a round hollow tube with sharp edges. - A saucerization biopsy removes the entire lesion by cutting under the lesion in a “scoop like” manner. This leaves a large, deep depression in the skin, but can be performed immediately and provides the
dermatopathologist with a complete specimen to better analyze the tumors architecture. - A fine-needle aspiration biopsy is done with a very thin needle and syringe that looks like a hypodermic syringe used for giving injections. It removes a very small sample of tissue. This type of biopsy is not done on a suspicious
mole or skin growth. Rather, it is done on other deeper tissue, such as nearbylymph nodes or an internal organ, to see if melanoma has spread.
Melanoma can spread quickly and produce large
Treatment of a primary lung or liver cancer is very different from treatment of melanoma that has spread to the liver or lung. That’s why it is important to find out if cancer in an organ is primary cancer or a malignant melanoma that has spread there.
|
How-To Information: How To Get A Second Opinion
Some people diagnosed with melanoma want to get a second opinion from a physician outside their treatment team. They ask a specialist in treating melanoma to review their diagnosis and treatment plan and offer suggestions. Doctors do not feel insulted or angry when patients ask for a second opinion from an outside specialist. Most are eager to cooperate. Indeed, some health insurance companies require a second opinion and many will reimburse the cost of getting one. There are many ways of finding a doctor to give a second opinion:
Getting a second opinion may delay the start of treatment for a short period, perhaps a week or two. It is unlikely that such a delay will affect the chances of being cured. |

Stages Of Melanoma
If a biopsy shows melanoma, it is important for the doctor to determine what stage it has reached before deciding on treatment. Staging involves measuring the thickness of the original tumor and checking to see if it has spread elsewhere. This may require additional tests, including blood tests, chest x-rays, and scans of the bones, liver, and brain.
- At first melanoma is limited, or localized, to one small place in the body. The tumor is relatively small and thin. Melanoma diagnosed at this early stage usually is growing only in the area of the visible tumor.
- In more advanced stages of melanoma, the tumor goes deeper into the skin and covers a wider area. It may spread, or
metastasize , generally tolymph nodes in the armpit, groin, or other parts of the body. - In the most advanced stage, the cancer has spread to other organs in the body.
What Factors Are Included In Staging?
What Is The Relationship Between The Stage And Chances of a Cure?
Why Are The Lymph Nodes Important In Diagnosing And Staging Melanoma?
Why Is Staging Important?
The doctor must know the stage of a cancer in order to pick the most effective treatment. Advanced cancer that has spread needs treatment very different from localized cancer growing only in the original tumor site. Staging also helps determine the
- Thin melanomas have a more favorable prognosis than thick melanomas.
- Melanomas that have not spread beyond the original tumor site have a much better prognosis than tumors that have spread to internal organs.
- If a melanoma is less than 1 millimeter (about 1/25 of an inch) deep, there is only a small chance that it has spread internally. The chances of spread are greater if a melanoma has grown thicker than 1.5 millimeters (about 1/6 of an inch).
Doctors use two terms to describe the thickness of a melanoma.

The
The Clark level. This uses a scale of I to V to describe a melanoma’s depth of invasion. Clark level is not based on a measurement, but on the number of layers of skin that the tumor has penetrated.
- Clark Level I tumors are still in the
epidermis , the outer layer of skin. These are called in-situ lesions. - Clark Level II and III tumors have spread to the upper part of the
dermis . - Clark Level IV tumors have reached the lower part of the dermis.
- Clark Level V tumors have penetrated into the fatty layer of the skin.
What Factors Are Included In Staging?
Staging of a melanoma takes into account the tumor’s thickness, whether it has spread, and how far it has spread. Melanomas generally first spread to nearby lymph nodes. A melanoma on the arm or chest, for instance, may shed cells that go to lymph nodes in the armpit.
The most widely used staging system is the
- T stands for tumor thickness and how far it has spread.
- N stands for lymph nodes, and whether the tumor has spread to the nodes.
- M stands of metastasis, and whether the tumor has spread to distant organs.
The TNM system combines information on all three factors to rank a melanoma in stages ranging from 0 to IV:
|
STAGE |
DESCRIPTION |
COMMENTS |
|
Stage 0 melanoma. |
Cancer cells are found only in the epidermis, the outer layer of the skin. |
This is the earliest and most curable stage of melanoma. Doctors may call it Clark Level I melanoma or in-situ melanoma. |
|
Stage I melanoma. |
Cancer has spread to the top of the dermis, but not to lymph nodes. The tumor is less than 1.5 millimeters thick. |
With the Clark system, such a tumor would be Clark Level II or III. |
|
Stage II melanoma. |
Cancer has spread to the bottom part of the dermis, but not to tissue below the skin or to lymph nodes. The tumor is larger, with a Breslow thickness ranging from 1.5 millimeters to 4 millimeters. |
It would be a Clark Level IV or V. |
|
Stage III melanoma. |
Cancer has spread to lymph nodes near the tumor site. |
|
|
Stage IV melanoma. |
Cancer has spread beyond nearby lymph nodes to internal organs. |
When |
What Is The Relationship Between The Stage And Chances of a Cure?
Doctors often measure the success of cancer treatment in terms of the five-year survival rate. A person usually is considered cured if he or she is alive and free of any trace of cancer five years after first being diagnosed.
The chances of a cure depend on many factors. One of the most important is the stage of the melanoma when it is diagnosed and treated.
The estimated five-year survival rates for melanoma by stage are:
|
STAGE |
SURVIVAL RATE |
|
Stage 0 |
virtually 100% |
|
Stage I |
over 90% |
|
Stage II |
about 80% |
|
Stage III |
about 50% |
|
Stage IV |
about 20% |
The actual outlook for an individual diagnosed with melanoma today may be better than these survival rates suggest. Constant advances in diagnosis and treatment of melanoma make the outlook brighter for today’s patients. More current survival rates are now being calculated.
Why Are The Lymph Nodes Important In Diagnosing And Staging Melanoma?
During diagnosis and staging of melanoma, the doctor routinely checks lymph nodes to see if they feel unusually large or hard, indicating that melanoma may have spread there.
If the doctor finds some lymph nodes that are hard or swollen, a fine-needle biopsy or actual removal of the suspicious nodes will be done. A
|
Need To Know: The Located along lymph vessels are lymph nodes, small knots of tissue about the size of a bean that filter the lymph. Nodes contain special cells that fight infections and trap cancer cells. While lymphatic vessels and nodes are found throughout the body, clusters of nodes are located in the neck, armpits, above the groin, and near some organs and large blood vessels. The lymphatic system can be a factor in the spread of melanoma because it does the following:
|
How Are Lymph Nodes Checked For Cancer Cells?
A relatively new procedure called
After an hour, the lymph nodes in the area of the
Targeting the sentinel nodes can avoid unnecessary removal of lymph nodes and related complications such as
How Is Melanoma Treated?
Treatment of melanoma depends on the disease stage, the individual’s age, overall health, and other factors. Doctors usually develop an individualized treatment plan for each patient.
Melanoma treatment often requires a team of specialists. The team may include:
- A dermatologis/dermatologic surgeon (skin specialist)
- A surgeon
- A plastic and reconstructive surgeon
- A medical oncologist (cancer specialist)
Generally one doctor takes responsibility for coordinating care.
Some people with melanoma decide to get a second opinion. They want another doctor to review the diagnosis and treatment plan and make suggestions. A second opinion can be especially important for individuals with melanoma that has spread and is in an advanced stage.
Surgery to remove the
When melanoma is more advanced, other treatments such as
In very advanced cases, surgery may not be helpful. The doctor may use only chemotherapy or other treatment methods.
Four kinds of treatment are used for most skin cancers:
In addition, some people explore other treatment options.
Surgery

Surgery involves removing the tumor and a wide margin of surrounding healthy tissue to reduce the risk that cancer cells are left behind in the area. The amount of surrounding tissue removed depends on the thickness and size of the melanoma. In some cases, the excisional
However, many people need surgery after the biopsy to remove tissue from the edges, or margin, of the tumor. If a wide margin of tissue must be removed, surgical treatment may also include a
Surgical treatment of larger, more advanced melanoma may include therapeutic
Chemotherapy
Chemotherapy involves the use of specialized drugs to kill the cancer cells. For treating melanoma, chemotherapy is given in a pill, injected into the body or given intravenously.
If the melanoma is more advanced, chemotherapy may be administered intravenously through a needle in a vein. This is called “systemic chemotherapy” and can kill cancer cells outside the skin. It may cause nausea and other side effects in some people. Side effects often are mild and usually can be controlled.
Biological Therapy
Biological therapy, or immunotherapy, uses the body’s own natural defenses to help attack and destroy melanoma cells. One form of biological therapy uses cancer-fighting substances that the body makes in small amounts. Larger amounts of the materials are produced in a laboratory and given to the patient. These substances are called biological response modifiers (BRMs).
BRMs include colony-stimulating factors, tumor vaccines, interleukin-2, or interferon-alfa. Biological therapy is used mainly for advanced forms of cancer that cannot be treated with other methods. In some cases, biological therapy is used after surgery to help prevent melanoma from recurring.
Radiation Therapy
This form of treatment uses energy from x-rays or other sources to destroy cancer cells. For melanoma, it usually helps to relieve symptoms that occur when cancer has spread elsewhere in the body.
For further information about radiation therapy, go to Radiation Therapy.
Are There Other Treatment Options For Melanoma?
People with melanoma can choose between standard therapy and experimental therapy. Standard therapy is the traditional treatment used by most doctors. Most standard treatments have been in use for years. Standard therapy, however, may not work for all people because it may not cure the disease or it may cause too many side effects.
In such cases, people with melanoma may benefit from experimental therapy. These are newer treatments that scientists are studying in clinical trials. In clinical trials, new treatments are tested on people to see if they are safe and effective.
Clinical trials can give cancer patients access to the newest and most hopeful scientific discoveries. The drawbacks of clinical trials are:
- Experimental therapy may prove less effective than more proven therapies.
- Experimental therapies may have side effects that have not been discovered yet.
Discussions with the doctor are important in deciding if a
|
Need to Know: A thorough investigation is necessary to decide whether a clinical trial is an appropriate treatment option. For a list of clinical trials, with locations and contact information, visit the clinical trials Web site. http://clinicaltrials.gov |
What Kind Of Follow-Up Care Is Needed After Treatment?
People treated for melanoma should see the doctor for regular checkups because they have a high risk of getting melanoma again. They may develop new melanomas or the old melanoma might recur in the original site or in new places in the body. The risk of recurrence is higher for people with thick melanomas or melanomas that spread to other areas of the body.
Regular follow-up care increases the chances that new melanomas will be found in an early and potentially more curable stage. Follow-up visits include:
- Thorough review of systems and general examination
- Thorough examination of the skin
- Possible blood tests and x-rays
- Possible scans of the bones, liver, lungs, and brain
|
Nice To Know: Q. How often should I return to the doctor for follow-up care after treatment for melanoma? A. That depends on the stage of your melanoma and a lot of other individual factors. Doctors usually ask patients to return for a complete checkup every three months for the first two years after treatment. Each visit will probably include a complete skin examination, and a check for enlarged Q. My wife was treated for melanoma. The A. Melanoma detected in an early stage often can be cured with the excisional biopsy-assuming a margin of normal surrounding tissue was removed (e.g. 5 mm of an in-situ melanoma) consonant with national guidelines. The excisional biopsy removes all the cancer cells before the melanoma has had a chance to spread to other organs. If your wife had Stage I melanoma, the doctor seems to be following national guidelines on melanoma care. These guidelines state that extra tests or treatment are not needed for very early melanoma. |
What Kind Of Follow-Up Care Is Needed After Treatment of Melanoma?
People treated for melanoma should see the doctor for regular checkups because they have a high risk of getting melanoma again. They may develop new melanomas or the old melanoma might recur in the original site or in new places in the body. The risk of recurrence is higher for people with thick melanomas or melanomas that spread to other areas of the body.
Regular follow-up care increases the chances that new melanomas will be found in an early and potentially more curable stage. Follow-up visits include:
- Thorough review of systems and general examination
- Thorough examination of the skin
- Possible blood tests and x-rays
- Possible scans of the bones, liver, lungs, and brain
|
Nice To Know: Q. How often should I return to the doctor for follow-up care after treatment for melanoma? A. That depends on the stage of your melanoma and a lot of other individual factors. Doctors usually ask patients to return for a complete checkup every three months for the first two years after treatment. Each visit will probably include a complete skin examination, and a check for enlarged Q. My wife was treated for melanoma. The A. Melanoma detected in an early stage often can be cured with the excisional biopsy-assuming a margin of normal surrounding tissue was removed (e.g. 5 mm of an in-situ melanoma) consonant with national guidelines. The excisional biopsy removes all the cancer cells before the melanoma has had a chance to spread to other organs. If your wife had Stage I melanoma, the doctor seems to be following national guidelines on melanoma care. These guidelines state that extra tests or treatment are not needed for very early melanoma. |
What Is The Best Way To Prevent Melanoma?
The most important way to prevent melanoma is avoiding excessive sun exposure. Prevention must begin in childhood, because most people get about 80 percent of their lifetime sun exposure before age 18.
Keep these facts about sun exposure in mind:
- Regular, day-to-day exposure is usually experienced by outdoor workers and individuals who spend lots of time in outdoor activities over the course of many years.
- Rare periods of intense exposure are often experienced by people who stay indoors most of the time and then sun themselves daily for a week or so while on vacation.
|
How-To Information: Practical prevention measures can help reduce the chances of developing skin cancer.
|
What Is The Outlook For Melanoma?
Scientists feel both concern and optimism about melanoma. Some think that thinning of the earth’s protective ozone layer may cause more cases of skin cancer in the future. The ozone layer is a band of gas high in the atmosphere. It filters some UV radiation from sunlight. Industrial chemicals, now banned in the United States and some other countries, caused the layer to become thinner in the past. Because of this, more UV rays reach the earth’s surface, raising skin cancer risks.
What is most important, however, is early detection. Melanoma detected and treated at its earliest stage is virtually 100 percent curable. That’s why regular skin self-examination and yearly skin examination by a trained professional is vital.
There is hope for reducing melanoma rates:
- Public education campaigns have increased awareness about the importance of prevention and early detection.
- Scientists are learning more about what causes melanoma.
- New advances in diagnosis,
staging , and treating melanoma offer more tools for curing this form of cancer.
Are There New Diagnostic And Treatment Discoveries?
One of the most promising new discoveries in melanoma treatment is gene therapy, replacing an abnormal gene, like the p16 gene, with a normal copy. Clinical trials of certain forms of gene therapy already are underway.
Advances in genetics research are leading to better methods for staging melanoma to help doctors pick the right treatment:
- New methods such as
lymph node mapping and sentinellymph nodebiopsy can more accurately indicate when melanoma has spread from its original location. - Newly developed “molecular staging” is more sensitive than staging done with a microscope. This technique can spot just one melanoma cell hidden among one million normal cells in the lymph node.
- These methods can avoid needless removal of
lymph nodes and complications such aslymphedema . At the same time, they can better determine when cancer cells have spread to the lymph nodes.
Melanoma: Frequently Asked Questions
Here are some frequently asked questions related to melanoma.
Q: How can I tell if a skin growth is melanoma? Is there any special appearance that I should watch for?
A: Be alert for growths that ooze fluid or blood, crust or clot over, and then ooze or bleed again. A sore that doesn’t heal after a week or two may be cancerous. Be on the lookout for moles or skin spots that are:
- Bigger from edge to edge than a pencil eraser
- Have uneven or ragged edges
- Show combinations of more than one color especially red, white and blue/black
- Have a different appearance on one half than on the other
Those are warning signs of possible melanoma. Check with the doctor if they occur.
Q: My wife was treated for melanoma. The
A: Melanoma detected in an early stage often can be cured with an excisional biopsy. The biopsy removes all the cancer cells before the melanoma has had a chance to spread to other organs. If your wife had Stage I melanoma, the doctor seems to be following national guidelines on melanoma care if he removed a margin of normal tissue (e.g. 5 mm for in-situ melanoma). These guidelines state that extra tests or treatment are not needed for very early melanoma.
Q: How can I tell if the treatment planned by local doctors is right for me? I have advanced melanoma that has spread to my
A: Get a second opinion. Have a melanoma specialist from another institution look over your treatment plan and offer suggestions. A lot of patients think their doctor will be insulted or angry if they ask for a second opinion. That’s rarely the case, however. A second opinion can benefit the patient and the doctors. Your doctor can refer you to a specialist for a second opinion. Names of melanoma specialists also are available from medical schools, local medical societies, and other sources.
Q: My friend read about a melanoma test that can show whether melanoma has spread to lymph nodes, and can pick out the exact nodes that have cancer cells. Should I ask the doctor about this test?
A: The test is a sentinel
Q: What’s
A: Lymphedema is a backup of lymph, the clear fluid that flows from tissues in the body to lymph nodes. From the nodes, lymph drains into the bloodstream. When all of the lymph nodes in the armpit are removed, lymph accumulates and may cause painful swelling and other problems in the arm. Lymphedema is a lot less serious than cancer, of course. Sometimes it can be avoided.
Q: How often should I return to the doctor for follow-up care after treatment for melanoma?
A: That depends on the stage of your melanoma and a lot of other individual factors. Doctors usually ask patients to return for a complete checkup every three months for the first two years after treatment. Each visit will probably include a complete skin examination, and a check for enlarged lymph nodes. Doctors may order a chest x-ray and scans of the lungs, brain, and other organs depending on symptoms.
Q: I’ve been referred to a dermatologist by my family doctor. She thinks that a growth on my back may be
A: It’s important to ask questions and work with the doctor in planning treatment and follow-up care. Start the dialogue by asking about the melanoma’s stage and whether to be concerned that the cancer has spread. Some other important questions include:
- What tests should be done, if any, to see if the melanoma has spread?
- What is the usual treatment?
- Will treatment cure the cancer?
- How often will I come back for follow-up care?
- What can I do to reduce my risk of getting skin cancer again?
Q: My mother had melanoma. I’m worried that I may get it, too, especially because I have a lot of moles on my skin. What kind of medical checkups are recommended?
A: Melanoma does run in families. If your parents had melanoma, your own risk may be higher than normal – especially if you have many moles of a certain kind. Your primary care doctor or dermatologist should do a total skin examination at each routine physical examination. That involves inspecting every inch of your skin, including the genital region and the area between the buttocks. If the doctor spots suspicious growths, you’ll probably get a referral to a dermatologist. Once you know that your skin is normal, get in the habit of doing a skin self-examination to watch for new growths or changes in existing growths.
Q: What is the best way of preventing melanoma?
A: Scientists don’t know for certain what causes melanoma. Many believe that too much exposure to the sun is the number-one cause. Try to avoid two kinds of exposure:
- Constant day-to-day exposure that occurs in people who work outdoors or enjoy outdoor sports or leisure activities.
- Less frequent but more intense exposure that causes sunburn. Vacationers, skiers, and others who get intense sun exposure a few times a year may be at high risk for
malignant melanoma, the most serious kind of skin cancer.
When you are in the sun, wear clothing that shields the skin. A broad-brimmed hat is ideal in the summer. Be sure to use a “broad-spectrum”
Q: If melanoma occurs mainly in people over age 50, why is it important for children to avoid getting too much sun?
A: Childhood sun exposure may set the stage for adult skin cancer. The average person gets about 80 percent of his or her total lifetime sun exposure by age 18. Most severe sunburns also occur during childhood and adolescence. A single severe sunburn in childhood may increase an individual’s risk of skin cancer.
Q: Can malignant melanoma occur anywhere else on the body?
A: Although most pigment-producing cells are in the skin, some
Melanoma: Putting It All Together
Here is a summary of the important facts and information related to melanoma.
Malignant melanoma is a rare but serious form of skin cancer. It is caused primarily by excessive exposure to ultraviolet (UV) rays from the sun – especially sunburn.- The incidence of melanoma can run in families. Individuals can have a predisposition to develop skin cancer.
- Anyone can get malignant melanoma. Risk factors include family history of melanoma, number and type of moles, personal history of melanoma, excessive exposure to the sun, severe sunburns, use of drugs that suppress the immune system, and advanced age.
- Changes in moles or freckles can indicate skin cancer.
- Melanomas are most often identified by the individual through skin self-examination or by a doctor during a routine physical examination. A
biopsy is the only way to confirm the presence of melanoma. - Melanoma that is diagnosed and treated very early has an excellent cure rate. However, melanoma can rapidly spread into lower layers of the skin, then to
lymph nodes and internal organs. - Melanoma is often painless and usually produces only two signs: a change in the size, color, shape, or feel of an existing
mole , and/or the appearance of a new growth or mole on the skin. - Most skin cancers that are diagnosed in the early stages can be treated with surgery.
Chemotherapy , biological therapy, andradiation therapy can be used if the cancer has moved into the more advanced stages. People with melanoma may also choose to participate in clinical trials of experimental therapies. - Once a person has had melanoma, she or he should continue with regular self-examinations and medical checkups.
- Melanoma can be prevented by limiting exposure to the sun’s harmful
ultraviolet rays . Practical prevention measures include avoiding sunburns, avoiding overexposure to direct and reflected sunlight, shielding the skin from the sun with clothing and hats, and using broad-spectrumsunscreen with a high SPF. - Melanoma has a high cure rate if it is diagnosed in the earliest stage.
- A routine skin self-examination is important for early detection of melanoma and in follow-up care of individuals treated for melanoma.
- Some people may inherit an abnormal gene from their parents that increases the risk of melanoma.
- Scientists don’t know for certain whether the use of sunscreen prevents melanoma, but it does protect the skin from the harmful UV rays that cause the cancer.
- Determining the stage of melanoma is important in selecting the best treatment.
Melanoma: Glossary
Here are definitions of medical terms related to melanoma.
Adjuvant therapy: Treatment given in addition to surgery for melanoma; it may include chemotherapy, radiation therapy, or immunotherapy
Basal cell carcinoma: Skin cancer that involves cells in the lower part, or base, of the epidermis (the outer layer of skin)
Benign: A growth that is not cancerous
Biological response modifiers (BRMs): Natural substances like interferon that are sometimes used to treat advanced melanomas
Breslow measurement: The actual thickness of a melanoma measured with a tiny device under a microscope that is used to stage melanoma
Biopsy: Removal and examination of cells or tissue under a microscope to check for cancer
Chemotherapy: Treatment with anti-cancer drugs
Clarke level: The depth into the skin to which a melanoma has grown; used to stage melanoma
Clinical trial: A research study done on human volunteers to decide if a new treatment is safe and effective
Cutaneous melanoma: Melanoma that starts in the skin, rather than the eye or an internal organ
Dermatologist: A medical doctor who specializes in diagnosis and treatment of skin cancer and other skin diseases
Dermatopathologist: A pathologist with special training and expertise in diagnosing skin cancer
Dermis: The middle layer of skin, located under the epidermis
DNA: Deoxyribonucleic acid, the substance within the genes that carries the genetic instructions
Dysplastic nevus: A mole with an unusual appearance; different from common moles
Epidermis: The outermost layer of skin, which is in contact with the environment, located above the dermis
Genes: The units of heredity that are passed from parent to offspring; genes determine particular traits in the individual, such as hair color or a propensity for cancer
Immunotherapy: Use of natural proteins produced in the body to fight melanoma
Lymph: Straw-colored fluid containing disease-fighting substances that flows through special channels in the body to the lymph nodes
Lymphatic system: The network of vessels and nodes returning lymph from body tissues to the bloodstream; the lymphatic systems is one of the body’s cleansing mechanisms and defends against infections
Lymphedema: Swelling of a limb that can occur when lymph nodes are removed or treated with radiation therapy
Lymph nodes: Small knots of tissue, about the size of a bean, that help fight disease; they are found in the underarms, chest, groin and other areas of the body, and contain special cells that fight infections and trap cancer cells
Lymph node mapping: Injecting a dye or radioactive substance into the body near the tumor site to identify the lymph node basin draining the tumor site and removing the first node in the basin, also called the sentinel node
Malignant: A cancerous growth that may destroy nearby normal tissue and spread to other parts of the body
Medical oncologist: A physician who specializes in the treatment of cancer
Melanocytes: Skin cells that produce a pigment called melanin; these cells can become cancerous and change into malignant melanoma
Melanoma: Cancer that occurs in melanocytes and is the most serious kind of skin cancer
Metastasize: The spread of cancer cells from the original tumor to distant parts of the body
Mole: A small, usually dark, skin growth that develops from pigment-producing cells called melanocytes
Nevus: The commonly used medical term for a mole (the plural is nevi); birthmarks are also called nevus or nevi
Ocular melanoma: Melanoma that begins inside the eye
Pathologist: A doctor who helps diagnose disease by examining cells and tissues under a microscope
Primary cancer: Cancer in the part of the body where it began
Prognosis: The patient’s outlook for recovering from a disease
Radiation therapy: Treatment that uses x-rays and other sources of radiation to kill cancer cells
Recur: When cancer returns after treatment to the same site or a new site in the body
Sentinel node biopsy: A procedure whereby the first node in the draining lymphatic basin is removed and examined by a pathologist for cancer cells
Skin graft: A patch of skin removed from one part of the body and used to cover another, such as an area from which a large melanoma has been removed
Squamous cell carcinoma: Cancer that occurs in squamous cells, the main cells of the epidermis (outer layer of the skin)
Staging: Determining the stage or extent to which a cancer has advanced
Sunscreen: A lotion or oil that helps protects the skin from harmful ultraviolet radiation, premature aging, and skin cancer
TNM system: A way of deciding the stage of a melanoma based on the tumor (T) size, whether it has spread to the lymph nodes (N), and metastasized (M) (spread to internal organs)
Topical chemotherapy: Treatment with anticancer drugs in a cream or solution applied to the skin over a period of time
Tumor: An abnormal growth of tissue that can be either benign (noncancerous) or malignant (cancerous)
Ultraviolet rays: Invisible rays in sunlight that cause suntan, sunburn, premature skin aging, and most cases of skin cancer
Melanoma: Additional Sources Of Information
Here are some reliable sources that can provide more information on melanoma.
American Cancer Society (ACS)
Phone: (800) ACS-2345 (toll-free hotline)
www.cancer.org
National Cancer Institute (NCI), Cancer Information Service
Phone: (800) 4-CANCER
Phone: 800-422-6237
www.nci.nih.gov
American Academy of Dermatology
Phone: 1-888-462-3376
Phone: 1-847-330-0230
http://www.aad.org
National Coalition for Cancer Survivorship
Phone: Phone:(877) NCCS YES
Phone: (877-622-7937)
Fax: Fax: (301) 565-9670
Email: info@cansearch.org
www.canceradvocacy.org