
In this Article
Glue Ear
What Is Glue Ear?
Glue ear is a painless condition in which thick, sticky fluid collects behind the eardrum. The fluid blocks the middle part of the ear and can cause impaired hearing. It usually affects children and is also known as:

- Chronic otitis media with effusion (OME)
- Secretory otitis media
- Middle-ear effusion
The thick fluid prevents normal movement of the small bones in the middle ear that are necessary for hearing. Glue ear is common in children because of the nature of their eustachian tubes, the tubes that connect the ears with the back of the throat.
Different kinds of fluid may be present behind the eardrum, ranging from a yellow liquid to a thick, white material that resembles glue (hence the name, glue ear).
Left untreated, glue ear can:
- Cause temporary hearing loss
- Contribute to delayed speech development in young children
- Affect a child’s behavior and educational progress
- In rare cases, cause permanent damage to hearing
About half of all cases of glue ear will resolve on their own within three months. About 90% of cases resolve within six months, and about 90% of cases resolve within three months. It is important to have the condition evaluated by a physician, because in the time it may take to resolve on its own, glue ear may affect a child’s speech development or behavior.
|
Need To Know: Having glue ear is like listening to the world with both fingers stuck in your ears. Children with glue ear cannot always hear everything that is said to them. But young children may not be able to explain the problem. Many become irritable and just want to be left alone. Any child who appears not to be hearing well should be evaluated by a physician and have a hearing test. |
|
Nice To Know: Q: How is glue ear different from an ear infection? A: Glue ear is not painful and does not cause the symptoms of a middle-ear infection (such as fever, crying, inability to sleep soundly, or tugging at the ear). Instead of pain, the child may experience a feeling of stuffiness in the ears and hearing loss. Glue ear may develop within weeks of an ear infection, but often the cause is unknown. |
Understanding How The Ear Works
The ear is divided into three parts: the outer ear, the middle ear, and the inner ear.

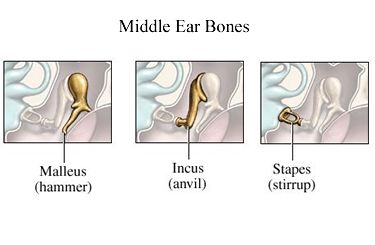
The middle ear is a small space between the outer and inner ear. It is separated from the outer ear by the eardrum. It contains three delicate bones (the hammer, anvil, and stirrup) that are important in hearing.
Here is how hearing works:
Sound creates vibrations in the air that are picked up by the eardrum.

When the eardrum vibrates, the tiny bones inside the middle ear also vibrate, transmitting the vibrations across the middle ear to the inner ear.

This causes fluid in the inner ear to move.
When fluid moves in the inner ear, it stimulates the nerve cells inside this part of the ear.

These nerve cells then send impulses to the brain along the “hearing nerve” (the cochlea nerve) and we then hear the sound.
A tube called the eustachian tube connects the middle ear to the back of the throat. When functioning properly, eustachian tubes do the following:
- Equalize air pressure on both sides of the eardrum. When you yawn or swallow and your ears “pop,” it is your eustachian tubes adjusting the air pressure in your middle ear. Negative air pressure in the middle ear causes pain and a “full” sensation in the ear.
- Allow drainage from the middle ear to the throat.
- Protect the middle ear from germs that may enter the back of the nose and throat.

|
Facts about glue ear
|
What Causes Glue Ear?
Glue ear occurs mostly due to a problem with the eustachian tube that connects the middle ear to back of the nose and throat.

The middle ear is normally filled with air that travels through the eustachian tubes to the back of the nose. The eustachian tubes equalize middle ear pressure and help drain fluids in the ear.
- If the eustachian tubes swell and block the drainage of the middle ear, air cannot enter the middle ear.
- When this happens, the cells lining the middle ear begin to produce fluid, which can become thick and glue-like as it fills the middle ear.
Children are especially prone to glue ear because:
- In babies and toddlers, the eustachian tubes are shorter and more horizontal than in an adult. This makes them less efficient to aerate the ear and more likely to become blocked.
- Children have frequent colds and sore throats because they have yet to build up useful immunity to common viruses, and this can affect the function of the eustachian tubes.
- In children, the adenoids (lymph tissue at the back of the nose that help protect against infection) are more likely to be enlarged, blocking the opening of the eustachian tubes.
|
Need To Know: Q: Are some children more likely than others to get glue ear? A: Some researchers believe children are at higher risk if they live in regions where there is cold weather, if they have frequent colds or |
|
Nice To Know: Some researchers have concluded that breast-feeding may reduce the chance of developing glue ear for babies and young children. They believe that breast milk contains proteins that have anti-inflammatory properties. These proteins may help to protect against glue ear even when breast-feeding has stopped. |
What Are The Symptoms Of Glue Ear?
Glue ear is not painful and can sometimes develop unnoticed. The symptoms of glue ear are:
- Temporary hearing loss. This is the most common symptom.
- A stuffy feeling in the ears. Glue ear does not cause pain the way middle ear infections (otitis media) can. Children most often will say they have a feeling of stuffiness or “fullness” in their ears.
Children with glue ear sometimes have repeated episodes of earache or middle ear infections.
In some children, the only sign of glue ear is a change in behavior. This may include:
- Becoming tired and frustrated
- Preferring to play alone
- Not responding when called
- Falling behind at school
Behavior changes can often be mistaken for stubbornness or rudeness. As a result, many children with glue ear are misunderstood or labeled as “difficult.”
How Is Glue Ear Diagnosed?
Because there often are no clear symptoms to suggest that your child has glue ear, your doctor may rely on one or several of these tests to make the diagnosis:

Otoscopy
Otoscopy involves looking at the eardrum using an instrument (called an otoscope) with a cone-shaped tip and a small light attached. The otoscope has a rubber bulb attached to see movement of the eardrum.The doctor may see signs of trapped fluid and poor movement of the eardrum. The eardrum will look clear and have no signs of redness, but will not move in response to the air, as a normal eardrum would.
Audiometry
Audiometry measures hearing across a range of frequencies. How this test is done depends on the age of the child. It usually involves having a child wear headphones and respond to a variety of sounds. There are now newer techniques for performing audiometry for very young children. However, some children with middle-ear fluid can have normal hearing.
Tympanometry
A tympanometry test is used to determine whether there is a problem with the middle ear. This test will evaluate the eardrum (tympanic membrane) by observing its motion in response to waves of pressure, and measuring the air pressure of the middle ear.
- A probe that your doctor will insert into the ear will emit a pure tone with a certain amount of sound energy. The probe measures how much sound energy bounces back off the eardrum, rather than being transmitted to the middle ear.
- The more energy returned to the probe, the stiffer and more blocked the middle ear is.
- Your child may feel some mild discomfort while the probe is in the ear, but the test is not risky.
An abnormal tympanometry test may indicate any of the following:
- Fluid in the middle ear
- A perforated ear drum or typanostomy tube
- Impacted ear wax
- Scarring of the eardrum
- A cyst growing in the middle ear
- Lack of contact between the bones of the middle ear that conduct sound
How Is Glue Ear Treated?
Glue ear does not always need treatment. Most physicians prefer a conservative, or “wait and see,” approach to treating glue ear.

- About 90% of cases resolve on their own within three or four months
Children who have complications such as frequent earache, or who might be at risk of developing speech problems because their glue ear is persistent, do need treatment.
The decision on whether or not to treat glue ear – as well as what type of treatment would be involved – is an individual one and requires discussion between parents and doctors. Treatment options include:
Antibiotics
The only medical treatment that has proven effective for glue ear is antibiotic therapy. But antibiotics are not always effective. A physician may prescribe antibiotics if:
- Infection is present
- The child is in pain
- There is evidence of hearing loss
Myringotomy
A procedure called a
A small incision is made in the eardrum to allow fluid to drain. The eardrum heals in about a week.
Myringotomy may also be performed to insert small ear tubes called tympanostomy tubes, or grommets, in the eardrum. These ear tubes allow the passage of air and aid further drainage of fluid.
Ear Tubes
Ear tube surgery, or tympanostomy, is performed in the hospital. Your child probably will be in the hospital for a total of two hours. Infants under 3 months may stay overnight. Here’s what to expect:
- Ear tube surgery will be performed in the operating room.
- Your child will receive
general anesthesia and will be asleep for about 10 minutes. - The surgeon will reach the eardrum through the external ear canal opening and will not cut the child’s skin.
- The surgeon will make a small hole in the eardrum to remove any fluid from the middle ear.
- The surgeon will insert a small metal or plastic tube into the hole in the eardrum to allow the remaining fluid and
bacteria to drain through the ear canal. - After ear tubes are placed, hearing almost always returns to normal, and the likelihood of your child having ear infections is greatly reduced.
- Ear tubes stay in the ear for about a year and then fall out on their own as the eardrum closes.
|
Nice To Know: Q: Are there risks involved in having ear tubes inserted? A. Placement of ear tubes must be done in the operating room, and this carries the usual risks associated with any general anesthesia. In a small number of cases, ear tubes don’t fall out on their own and must be surgically removed. Also rare are cases in which the ear tube falls out, but the hole in the eardrum left behind does not close up on its own. Surgery may be necessary to patch the hole. |
|
Nice To Know: If your child has ear tubes, be sure he or she uses earplugs or cotton balls coated in petroleum jelly (Vaseline) to keep water away from the eardrum. |
What Can I Do To Help My Child?
It is important that glue ear be identified as soon as possible. Until the condition is resolved, parents may wish to:

- Make teachers and the school nurse aware of the difficulties that glue ear can cause, especially behavioral issues and temporary hearing loss
- Suggest that the child be seated near the teacher in the classroom, in order to better understand what is being discussed in class
It also is important to ensure that children eat a balance diet, get enough exercise, and get enough sleep.
Some parents have found that cutting down on the amount of dairy products (such as milk, cream, and cheese) has helped in reducing the production of mucus in their child. But these foods are also sources of essential nutrients for children, so any reduction of dairy products should be replaced with adequate substitutes. Your child’s doctor can help with diet decisions.
|
How-To Information: Here are some basic communication tips:
|
|
Nice To Know: A pinch of relief To relieve a feeling of fullness in the ear, have your child try this simple trick: Take a deep breath, close the mouth, and try to blow air out through the nose while pinching its end firmly closed. This may help to equalize the pressure between the middle ear and the air outside after air travel, and may help open the |
Glue Ear: Frequently Asked Questions
Here are some frequently asked questions related to glue ear.
Q: How is glue ear different from an ear infection?
A: Glue ear is not painful and does not cause symptoms of a middle-ear infection (such as fever, crying, inability to sleep soundly, tugging at the ear). Instead of pain, the child may experience a feeling of stuffiness in the ears and hearing loss. Glue ear may develop within weeks of an ear infection, but often the cause is unknown.
Q: Are some children more likely than others to get glue ear?
A: Children with genetic conditions such as cleft palate or Down syndrome may have smaller
Q: Are there risks involved in having ear tubes inserted?
A: Placement of ear tubes must be done in the operating room, and this carries the usual risks associated with any
Q: My son just seems to hear when he wants to and often appears to be daydreaming. His teacher says he’s lazy, but I think he’s not hearing properly. Could he have glue ear?
A: Maybe. Because glue ear is not painful, often it is behavior problems that provide the first clue. When children have hearing difficulties, parents usually recognize or suspect something is wrong. Trust your own judgment, and have your child’s ears checked by a physician.
Glue Ear: Putting It All Together
Here is a summary of the important facts and information related to glue ear.
- Glue ear is a painless condition in which thick, sticky fluid collects behind the eardrum. The fluid blocks the middle part of the ear and can cause impaired hearing.
- Left untreated, glue ear can cause temporary hearing loss, contribute to delayed speech development in young children, affect a child’s behavior and educational progress, and in rare cases cause permanent damage to hearing.
- Glue ear can sometimes develop unnoticed. The most common symptoms are hearing loss and a stuffy feeling in the ears. In some children, behavior problems are the first clue.
- A physician can diagnose glue ear by looking inside the ear with a special instrument and conducting a hearing test (an otoscopy), and by using a test called tympanometry to determine if there is a problem with the middle ear.
- Glue ear often clears up on its own, without treatment.
- When treatment is necessary, the options include antibiotic medication, a procedure to drain the fluid called a
myringotomy , and the placement of ear tubes. - Parents can help children with glue ear by talking with teachers about the condition and by using basic communication tips – such as getting the child’s attention before beginning to speak and speaking clearly – to help the child understand what is being said.
Glue Ear: Glossary
Here are definitions of medical terms related to glue ear.
Allergy: An unusual response to a small amount of a foreign substance that normally does not cause a reaction in another person
Bacteria: Microscopic organisms; unlike viruses, they generally respond to antibiotics
Eustachian tubes: The tubes that connect the middle ear to the back of the throat; their function is to equalize the air pressure in the ear
General anesthesia: Putting a person to sleep for an operation
Glue ear: A painless condition in which thick, sticky fluid collects behind the eardrum, blocking the middle part of the ear and possibly causing impaired hearing
Myringotomy: A small incision made into the eardrum to allow fluid to drain from the ear
Tympanostomy tube: Plastic tube that is inserted into myringotomy
Virus: A microscopic organism; antibiotics have no effect on viruses
Glue Ear: Additional Sources Of Information
Here are some reliable sources that can provide more information on glue ear.
American Academy of Otolaryngology Head and Neck Surgery
http://www.entnet.org/
Ear Surgery Information Center
http://www.earsurgery.org/
Association for Research in Otolaryngology
www.aro.org
Books:
Bluestone, Charles D. Conquering Otitis Media.
Greene, Alan R. The Parent’s Complete Guide to Ear Infections.
Schmidt, Michael A., and Rapp, Doris. Healing Childhood Ear Infections; Prevention, Home Care, and Alternative Treatment.