
In this Article
Angina
What Causes Angina?
The coronary arteries are small arteries that carry blood to the heart muscle. This blood flow provides the oxygen and nutrients needed by the heart itself so that it can keep pumping. If the heart has to speed up (for example, during exercise or periods of excitement) and cannot get the blood it needs, it will send out a signal in the form of angina.
The three major coronary arteries are the:
- Left anterior descending artery
- Left circumflex artery
- Right
coronary artery
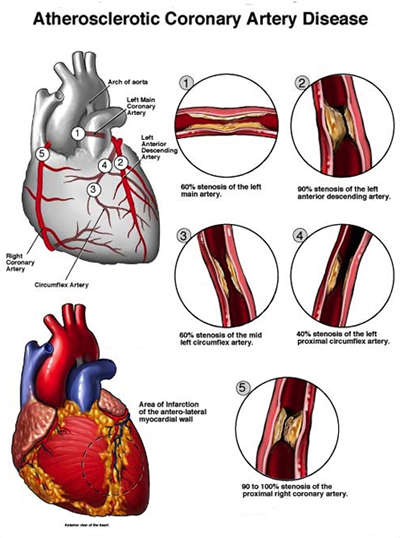
Most people with angina have blockages in one or more of these arteries and/or their branches. A cardiologist (heart specialist) will perform various tests to determine the location and extent of the blockage.
The two major causes of angina are:
- Coronary artery disease (CAD)
- Coronary artery spasm
In almost all cases, the underlying cause of angina is the critical narrowing of one or more of the coronary arteries that supply blood to the heart.
Coronary artery disease – also known as coronary heart disease (CHD) or ischemic heart disease (IHD) – affects most people as they age. The coronary arteries become constricted or blocked by atheromas – bulging masses or “plaques” that form within the walls lining the arteries.
Nice To Know:
“
The more atheromas that line the coronary arteries, the narrower the pathway for blood. Atherosclerosis often restricts as much as 70% of the blood that flows through the coronary arteries. Although the heart muscle receives enough blood for routine activities like walking or sitting,
Need To Know
Stable angina itself is not dangerous, but it does indicate the presence of underlying coronary heart disease. The plaques and narrowed coronary arteries that cause angina significantly increase the risk of a heart attack.
A heart attack occurs if a clot sticks in the narrowed part of a coronary artery and no blood can get through at all. Part of the heart muscle will die since it will not be supplied with the necessary oxygen to survive.
The exact cause(s) of coronary artery disease remains unknown. Yet experts have identified some of the risk factors that increase a person’s chance of getting this disease. They include:
- Aging
- High blood pressure (hypertension)
- Cigarette smoking
- High blood
cholesterol - Being overweight
- Lack of exercise
- Family history of angina or heart attack at a young age
- Diabetes
Certain individuals, though, develop angina without having any of the above common risk factors for CAD.
Coronary artery spasm
A more unusual type of angina is caused by spasm (sudden contraction [squeezing response]) of the smooth muscle within the coronary arteries. This condition is called
variant angina pectoris
(also known as “Prinzmetal’s angina” or angina inversa).
Variant angina pectoris does not occur when the heart has been overworked. Instead, variant angina comes on almost exclusively when a person is at rest or asleep, often between the hours of midnight and 8 a.m. The attacks can be extremely painful.
Variant angina is associated with coronary artery disease (CAD). About 65% of all sufferers have atherosclerosis in at least one major vessel of the heart. The coronary artery spasm that causes this form of angina typically occurs very near the atherosclerotic blockage.
People with variant angina often experience an active phase of the disease in which they are at particular risk for:
- Serious cardiac arrhythmias (heart rhythm disturbances), such as
ventricular tachycardia (rapid rate of the left, pumping chamber of the heart) andfibrillation (rapid, uncoordinated contraction [squeezing] of the heart muscle) - Myocardial infarction (MI; a heart attack)
- Sudden death
During this phase – which can last three to six months or more – an individual may experience frequent attacks of angina and