
In this Article
Knee Replacement
How Is The Knee Replaced?
Once the anesthetic has been given and the patient prepared: the damaged joint surfaces are removed. An incision approximately eight inches in length is made on the front of the knee.
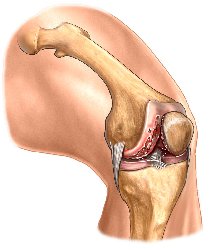
The damaged joint surfaces are removed from all 3 bones making up the knee joint. Sometimes, depending on the surgeon, the back of the knee cap is left intact if it is not badly affected by the arthritis. The surrounding muscles and most of the ligaments are preserved.

The lower end of the thigh bone (femur) is resurfaced with a metal cap.

The upper end of the leg bone (tibia) is replaced with a plastic and metal implant with cement and or screws.

The back of the kneecap (patella) is also resurfaced with an all-plastic implant. Highly specialized instruments are used that allow precision cutting of the bone so that the new joint fits perfectly. The type of implant used depends on surgeon’s preference and patient requirements.)
Recovery In The Hospital
The first days after total knee replacement
The first day you can expect:
- Diet may be clear liquids only
- Intravenous line in the arm for fluids and antibiotics
- Pain medication by injection, or intravenously or as tablets.
- Blood transfusion if necessary
- Activity as tolerated to include walking: (Full weight bearing if a cemented knee was used and toe touch or limited weight bearing if an uncemented knee was used).
- Breathing exercises
The second and third day you can expect:
- Exercise program initiated
The fourth day to one week you can expect:
- Progression of walking and exercises.
- Instruction on how to dress, get in and out of bed and utilize the bathroom safely.
Your Team

Postoperative care begins with a team approach of heath professionals within the hospital. Those closely involved with the postoperative total knee patient are:
The Nursing Staff
After surgery, vital signs and sensation in the lower extremities are observed and checked by the nursing staff and documented for the physician. Antibiotics are administered according to the physicians preference to reduce the risk of infection.
The surgical incision is observed closely for:
- Excessive drainage
- Proper initial healing
- The need for changing of sterile dressings
The Respiratory Therapist
The respiratory therapist is essential at this stage for:
- Instruction for coughing and deep breathing exercises to help prevent complications, such as congestion or pneumonia.
- Instruction on how use a bedside device to assist in deep breathing exercises called the Incentive Spirometer. This device along with deep breathing exercises are important to minimize the risk of lung complications after surgery by removing any excess secretions that may settle in the lungs while asleep during surgery.
The Physical Therapist
Shortly after surgery the physical therapist addresses:
- Circulation– At this point in the recovery, early stage exercises are instructed by the acute care physical therapist such as moving the ankles up and down to promote circulation and prevent clots. These exercises are often called ankle or gastrocnemius pumps.
- Range of motion– In order to aide the rehabilitation process at this stage, the physical therapist will place the operated leg in a
continuous passive motion (CPM) machine. This machine supports the leg while it slowly and gently bends and straightens the knee. This passive motion (motion performed by the machine not the patient) helps prevent stiffening and reduces postoperative scarring. It is not uncommon for this device to be started in the recovery room with the patient waking up from surgery finding their knee moving under the power of the CPM machine. - Mild muscle strengthening exercises -Once swelling has been stabilized and there is progress in the range of motion of the knee, mild strengthening and additional range of motion exercises are taught by the physical therapist to promote muscle activity and decrease muscle loss, which can occur with inactivity.
- Gait training-The physical therapist helps get you walking, beginning with short distances using crutches or a walker. This not only promotes the ability to bend the knee and strength but is also important for endurance and stamina. It is critical not to take full weight through the leg if those were the instructions given.
The Occupational Therapist
The occupational therapist is involved in evaluating and addressing how well the patient with the new knee replacement functions with activities of daily living. Issues such as how safely and independently the patient is able to dress, bathe, and care for his or herself following total knee replacement are evaluated.