
In this Article
Osteoarthritis
What Is Osteoarthritis?
The word arthritis literally means “joint inflammation” – that is, a joint that is painful, warm to the touch, possibly red, swollen, and associated with a loss of function. “Osteo” is Greek for “bone”.

Arthritis is not a single ailment. In fact, more than 100 different conditions can affect the joints and their adjacent bones, muscles, and tissues. They are classified into various major types of arthritis, depending on whether or not inflammation, infection or bleeding is the major component. All of these types of arthritis are completely different, with different presentations, symptoms and treatment.
Osteoarthritis (OA) is the most common form of arthritis.
It is a ‘non-inflammatory’ type of arthritis, which means that inflammation is not the key component. It is completely different from the less commonrheumatoid arthritis, which is an inflammatory arthritis in which the body’s immune system attacks its own tissues, causing joint damage.

- The causes and treatments of these other arthritis-related diseases differ from OA.
- While OA sometimes may be painful, it is not always disabling, and unlike rheumatoid arthritis, is unlikely to produce severe deformity of the joints.
- Osteoarthritis can involve a number of joints, but it is not a disease that spreads to involve other tissues or joints throughout the body.
Osteoarthritis (OA) has been called a “degenerative” condition because it is caused, in part, by wear-and-tear of a joint over time. Its impact is significant:
- OA occurs in both men and women and usually develops after age 45.
- More than 16 million Americans, including over 50 percent of people over 65, have some degree of osteoarthritis.
- Older people often don’t realize that they have OA if they are free of pain and other symptoms. However, x-rays often reveal some OA of the spine or fingers in elderly individuals.

Osteoarthritis develops in a joint when
- Prolonged “wear-and-tear” as we age
- Prior injury or damage to the joint from trauma or infection
- Cartilage that is altered by other disease or is genetically weak.
But in most cases we simply don’t know what causes it.
Unfortunately, damaged cartilage cannot heal to become normal again, though tremendous research is underway developing methods to restore damaged cartilage.
How It Progresses
Here is how OA progresses:
- The smooth cartilage that lines and protects the bone ends begins to retain water, and changes occur in some of the chemical substances that make up the cartilage
- Tiny cracks develop in the cartilage, which then splits further forming clefts and fissures
- The ends of the bones begin to thicken and grow out from the joint margin. These small bone growths are called osteophytes or “
spurs “. Actually, these spurs are nature’s way of trying to help the damaged joint by allowing the load through the joint to be redistributed. But these bony outgrowths often interfere with the mechanism of joint movement. - Cysts, which are small cavities, develop in the bone just beneath the damaged cartilage
- Fragments of damaged cartilage or bone may break off and float around freely in the joint as ‘loose bodies’ and may cause additional problems.
- As the cartilage becomes more damaged, the joint space becomes narrower and narrower.
- The damage to cartilage within a joint can irritate and inflame the inner lining of the joint called the
synovial membrane and cause it to produce excess fluid. It normally produces a lubricant calledsynovial fluid , which helps to lessen friction in the joint.The fluid may then build up within the joint and lead to detectable swelling.
When the cushioning system of the joint is lost, the bones may grind painfully against each other. The joint can begin to stiffen, and movement is impaired.
Some people are fortunate in that despite having these rather severe osteoarthritis changes in a joint, they experience very little, or no pain at all.
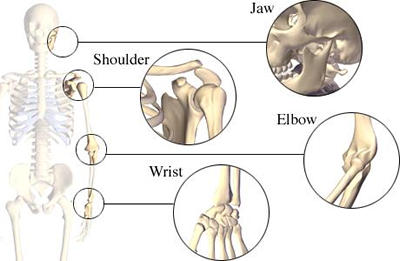
Osteoarthritis typically strikes the:

- Weight-bearing joints (knees, hips, back, feet)
- Hands
- Spine
The knee is the most commonly affected joint.
If osteoarthritis develops in the hips or knees, it often occurs in only one joint but may affect any number of joints.
If the hands are affected, a few finger joints may become arthritic at the same time.
- Bony lumps that arise in the middle finger joints are called
Bouchard’s nodes . - Lumps that arise in the last finger joints are called
Heberden’s nodes . Heberden’s nodes occur most often in women, who are also prone to experience osteoarthritis of the hands in general, as well as the knees.
|
Nice To Know: Q: What is the difference between osteoarthritis (OA) and rheumatoid arthritis (RA)? A: The principle features of the two conditions are not the same, and their treatment is very different. In OA, the cartilage in the joint becomes damaged and, ultimately, the joint degenerates. The joint is not primarily inflamed, although inflammation may occur as a late result. On the other hand, in RA, there is initial inflammation of the lining of the joint. This produces a soft, tender swelling in contrast to the bony enlargement of OA. Cartilage damage occurs later as a result of this inflammation. The pain of OA is often least troublesome in the morning but may gradually worsen during the day. With RA, the pain and stiffness usually is worst on waking, but gradually improves during the day. |
Rheumatoid arthritis is not just a disease of the joints, it is a systemic disease, meaning it affects the whole body. Abnormalities occur in the blood vessels, circulating cells and proteins, as well as connective tissue. Not surprisingly, RA is associated with more generalized disturbances – such as anemia (low red blood cell count) – which are proportional to the activity of the arthritis. Usually more than one joint is involved in RA, with the hands almost always affected.
|
Facts About Osteoarthritis
|
What Causes Osteoarthritis?
Despite years of research, no one has a simple answer to this question. Many factors probably cause the initial cartilage damage that sets off the destructive process. It remains a mystery why particular joints are affected by osteoarthritis (OA) if they have not suffered any previous injury or disease.

Joint Wear-And-Tear
The aging process clearly can contribute to the breakdown in the joints and cause osteoarthritis, but not all elderly people develop detectable OA. In addition, athletes and laborers often subject their joints to prolonged wear-and-tear, which places them at increased risk of developing arthritis in later years.
Joint Injury Or Overuse
Along with continual wear-and-tear, osteoarthritis has been linked with damaging events such as:
- Fractures and infections that can harm the internal tissues of a joint. Individuals who experience repeated knee injuries – such as basketball, football, or soccer players – are much more likely to develop osteoarthritis as they get older.
- In addition, people who overuse their joints by subjecting them to repeated stresses and strains are at increased risk. This is particularly evident in specific occupations such as jackhammer operators, who often develop arthritis of the hands or elbows, and ballet dancers, who develop arthritis of the feet.
Inactivity
Not surprisingly, physical inactivity can be as harmful to the joints as overuse. A lack of exercise or varied movement can weaken the muscles that support the joints and decrease joint flexibility. Eventually, an underused joint may become stiff, painful, dysfunctional, and prone to injury and osteoarthritis.
Excess Body Weight
Heavy individuals are at increased risk of developing arthritis because their joints may be strained by excess weight. This is especially evident in weight-bearing joints such as the knees and hips, which often show the first signs of weight-related strain and injury.
|
Nice To Know: Research indicates that people who are overweight as young adults are likely to develop osteoarthritis of the knee as they age. |
Since being overweight can increase the chances of joint damage and worsen arthritic symptoms, most experts recommend weight-loss programs for overweight people who are at risk for osteoarthritis. Weight gain also should be avoided to help prevent the arthritis that may occur with aging.
Heredity
Current research suggests that the
|
Nice To Know: Scientists have discovered an abnormality in a gene responsible for the production of |
Osteoarthritis of the fingers occurs very commonly in families and is most common in women.
In addition, OA is more likely to develop in people who are born with heredity defects that make their joints fit together incorrectly, such as:
- Bow legs
- A hip dislocation
- Laxity (double-jointedness)
What Are The Symptoms Of Osteoarthritis?
Depending on the joint affected, people with osteoarthritis may experience specific symptoms in the joints such as:
- Pain
- Stiffness
- Bony enlargement and swelling
Activities of daily living, such as climbing stairs or opening jars, often become more difficult as the joints become more affected by the disorder.
Osteoarthritis typically occurs in one or two joints at first, most frequently targeting weight-bearing joints that include:
- Hip
- Knee
- Spine
- Hands
- Small hand joints may also be involved.
Pain And Limitation Of Motion
The pain of osteoarthritis often manifests as a deep ache within or near the affected joint, coupled with a limitation of motion. In OA, most people typically experience joint pain that worsens during the course of the day, whereas others report the greatest pain in the morning (which is related to the symptom of stiffness after activity)
Osteoarthritic pain primarily is caused by joint damage.
- Joint pain results when bony overgrowths rub together or when small stress fractures are present.
- In addition, secondary injuries may occur if pain limits a joint’s normal range of motion.
- The body may respond by protectively “favoring” one joint over another. For example, if the painful joint is a knee or an ankle, the “favored” joint may be overused, causing painful muscle strain.
Other painful sensations, such as rubbing or grating within the joint, may be felt when a person performs specific activities such as:
- Bending
- Kneeling
- Stair climbing
As
|
Nice To Know: Pain does not come from the cartilage (which contains no nerves), but from the adjacent stretched or irritated tissues. |
Sometimes osteoarthritis can cause referred pain – that is, pain that is not experienced directly in the damaged joint, but is felt in other regions instead. For example:
- An arthritic hip joint may cause painful sensations in the buttocks, groin, thigh, or knee.
- Arthritis of the spine can cause pain that radiates to the neck, arms, or legs.
Osteoarthritic pain, like other pain, may worsen after stressful life events, such as the loss of a loved one or separation from a spouse.
Stiffness After Inactivity
After periods of inactivity (for example, sleeping or prolonged sitting), a person may experience considerable stiffness in the osteoarthritic joint. Stiffness usually lasts for about 30 minutes or less and is improved by mild activity that ‘warms up’ the joint.
|
How-To Information: Inflammatory arthritis, such as rheumatoid arthritis, is distinguished by joint stiffness that is most pronounced in the morning or after a period of inactivity.
|
Bony Enlargement And Swelling
Progressive breakdown of cartilage may lead to the formation of enlarged bony growths or “
Once the
Osteoarthritis usually doesn’t cause any prominent inflammation (a protective response in which tissue may become red, warm, and tender) in response to injury. This distinguishes it from rheumatoid arthritis, which is associated with considerable joint inflammation. Occasionally people with osteoarthritis experience mild inflammation, although the exact cause of this response remains unknown.
Diagnosing Osteoarthritis
A diagnosis of osteoarthritis is made with:
- A medical history and physical examination
- Imaging methods
- Laboratory tests

Physical Examination
A primary care physician or rheumatologist (specialist in rheumatic disorders of the joints and related structures) will ask about:
- Joint symptoms
- Previous or current illnesses
- Traumatic injuries
- Operations you may have had
- Allergies
- Other medical conditions
The physician will inspect the affected joint(s), checking for swelling, redness and heat, tender points, skin rashes, and other bodily signs. Determining which joints are involved and how their function is impaired helps the physician to distinguish OA from other forms of arthritis.
The muscles that surround painful, underused joints may show signs of weakness. The pattern of arthritis in the hands may be especially helpful in the diagnosis. OA tends to involve the base of the thumb and the middle and end joints of the digits.
Imaging Methods
X-rays will confirm the diagnosis of arthritis but will not necessarily indicate the type of arthritis. The physician will look for specific structural changes in the joint(s) that suggest OA, such as:
- Narrowing of the joint space. This occurs due to loss of
cartilage (for example, joint space narrowing of the inside half of the knee). - Bony
spurs . These are outgrowths of new bone called osteophytes that develop at the margin of the joint. It is nature’s way of protecting the joint. - One-sided distribution (for example, one knee, one hip) of joint irregularities.
- Cysts. These may be seen in the bone just beneath the joint surfaces.
By contrast, imaging studies in people with rheumatoid arthritis more often show
- Loss of calcium from the bone (localized bony decalcification)
- Erosion-producing defects or holes in the bones in a joint
- Changes in many joints on both sides of the body, particularly the hands and wrists
Laboratory Tests
If there is a question about the exact nature of joint swelling, the physician may perform a joint aspiration. During this procedure:
- A needle is gently inserted into the joint to withdraw a small amount of
synovial fluid from the joint. - The fluid then is tested for chemistry, viscosity (thickness), blood cell counts, overall appearance, and microorganisms (if an infection is suspected).
- The fluid from an OA joint is usually clear, whereas in RA, it is cloudy due to the presence of many white blood cells.
- The fluid then is tested for crystals to exclude such diagnoses as
gout . - Sometimes the fluid from an OA joint contains calcium pyrophosphate crystals, which may cause mild irritation and increase swelling.
Blood tests may be ordered in puzzling cases to identify infection, measure blood cell counts, and pinpoint telltale diagnostic findings such as rheumatoid factor (RF) and human leukocyte antigen (HLA-DR4 and HLA-DR1), which are more common in people with inflammatory types of arthritis such as rheumatoid arthritis.
Blood and urine tests may be ordered to rule out conditions such as gout. The blood from people with gout contains a high level of uric acid, which is associated with the buildup of arthritis-causing crystals in the joint fluid.
What Treatment Is available For Osteoarthritis?
Successful treatment programs are tailored to meet the needs of the individual.
By treating arthritis early and following a well-designed treatment plan, you can:
- Reduce your symptoms
- Increase joint movement
- Lessen joint-damaging effects
Osteoarthritic joints are not always painful, and when pain is present, it can vary in intensity. In some people severe osteoarthritis is completely pain-free, whereas in others even minor joint changes are quite painful.The response to arthritis pain is broad and very personal.
Because of this, it is important to have an individually designed treatment program. What works for one person may not necessarily work for another, even if both have osteoarthritis of the same joint.
Treatments include:
- Weight control
- Proper exercise
- Heat and cold therapy
- Pain medication
- Other pain relief options
- Stress control
- Injections into the joint
- Surgery
Weight Control
Weight control is important to successful arthritis management. Research suggests that:
- Being overweight is a risk factor for osteoarthritis
- Overweight young adults are likely to develop osteoarthritis of the knee as they age
Controlling your weight can:
- Lessen pain by reducing stress on the weight-bearing joints (hips, knees, back, feet)
- Increase self-esteem and avoid the risk of psychological suffering and/or depression that can affect overweight individuals
Weight loss should be coupled with a regimen of more physical activity. A productive goal is a total of 30 minutes of daily exercise. Exercise may need to be altered in the presence of OA, but most can exercise.
|
Nice To Know: Glucosamine and Chondroitin Glucosamine sulfate and chondroitin sulfate are two nutritional supplements that have been reported to “cure” arthritis.1 Because glucosamine and chondroitin are produced within the body and are used in the manufacture or repair of Preliminary reports indicate that glucosamine may indeed relieve the pain and stiffness of osteoarthritis, especially when combined with exercise, weight loss, physical therapy, and other measures. Unfortunately, there is limited information about the long-term effects of both supplements and their potential interactions. Some European studies have reported pain relief and increased movement in the knees of osteoarthritis patients who were treated with glucosamine sulfate or chondroitin sulfate. And, although the results are encouraging, these studies have not yet appeared as full-length papers in peer reviewed journals.
According to the Arthritis Foundation: “While European studies on glucosamine sulfate and chondroitin sulfate in the treatment of osteoarthritis of the knee are promising, the Arthritis Foundation cannot formulate a definite recommendation on the use of glucosamine sulfate or chondroitin sulfate in the treatment of osteoarthritis (OA) until more substantive data are available.”2 Glucosamine and chondroitin products – like all dietary supplements – are not subjected to the strict regulations of the Food and Drug Administration (FDA), so buyer beware. Arthritis sufferers should check with a physician before taking them, and, if glucosamine sulfate and/or chondroitin sulfate are already being used, report such use (and the use of any other nutritional supplements) to a physician. 1 Theodakis J, Adderly B, Fox, B: The Arthritis Cure. (New York: Affinity Communications Corp., St. Martin’s Press), 1997. 2 Arthritis Foundation, news release, 1998. |
Excerise
Regular exercise is very important for successful control of osteoarthritis.
Strengthening and stretching exercises can help by:
- Relieving pain and improving joint movement
- Building up the muscles around the joint, making the joint more stable and resisting further damage.
Specific exercises may be prescribed to improve strength and range of motion in particular joints and muscles. Three types of exercise are used to treat osteoarthritis:
- Stretching exercise
- Isometric exercise
- Aerobic (endurance) exercise
1. Stretching exercise. Also called range-of-motion (ROM) exercise, it helps to maintain joint flexibility and reach. It includes anything that puts a joint through its fullest range of motion (for example, stretching the shoulder joint by holding the arms out at the sides and circling them in a windmill fashion). Stretching exercise often is more easily performed if the person takes a pain reliever or applies heat to the joint before starting to exercise.
2. Isometric exercise. This is exercise in which muscles are tensed for a period without actually moving them. It can be performed without actually bending a painful joint. As muscles are exercised against resistance, their size and power will increase.
3. Aerobic exercise. This is endurance-building exercise that improves cardiopulmonary (heart/lung) fitness. For most individuals with osteoarthritis, the best aerobic exercises are:
- Swimming (especially in a heated pool)
- Walking on level ground
Such gentle exercises are less stressful on the joints. Water exercise is especially recommended for people who have osteoarthritis of the large joints (hips, knees). The buoyancy of the water makes it possible to exercise while the body weight is supported.
|
How-To Information: People with osteoarthritis of the weight-bearing joints should avoid activities such as jogging and tennis. These sports can put too much strain on the legs or require sharp turns and twisting movements. In addition, exercise bicycles should be used with caution by people with arthritic knees. |
Since pain may worsen with increased activity, people with advanced osteoarthritis may need to take several rest periods during the day. On the other hand, too much inactivity can worsen osteoarthritis by causing increasing stiffness. An optimal treatment plan should achieve a balance between daily exercise and adequate rest.
Heat And Cold Therapy
Heat and cold treatments are well-known to reduce the pain, stiffness, and occasional swelling associated with osteoarthritis. But this is generally temporary. There is no ‘set’ formula for therapy. Heat works better for some individuals, whereas others favor cold.
Heat often is used to relieve pain or relax muscles before the start of exercise.
- Heating pads or hot packs can be positioned over stiff joints. Some people prefer “moist heat” in the form of warm towels, a warm shower or bath, or a heated whirlpool or hot tub.
- Other heat treatments include ultrasound and immersion of painful hands into warm wax. All are able to bring soothing heat to sore joints.
- Heat should be applied at a comfortable temperature and seems to be most beneficial when used over the muscles adjacent to the joint.
Cold can lessen pain in a sore joint by numbing the local tissues.
- It may be applied in the form of a reusable pack or ice.
- Ice and cold packs never should be placed directly on the skin, as they are likely to cause skin damage. Instead, ice and cold packs should be wrapped in a towel before they are applied.
|
How-To Information: Safety tips:
|
Pain Medication
Medicines to control OA pain must be pain-specific, since osteoarthritis can cause both sudden and chronic pain.
- If a person experiences unexpected, severe pain from a damaged joint, he or she might benefit from strong pain relievers and muscle relaxants.
- By contrast, such medications usually are not useful or appropriate for chronic pain, which is more effectively treated by self-management techniques such as proper joint use, joint protection, exercise, medication scheduling, and weight control.
Many medications are used to treat arthritis. Some must be prescribed by a physician, whereas other “over-the-counter” (OTC) products can be bought without a prescription.
OTC pain relievers like acetaminophen (Tylenol®) and aspirin are familiar choices for the treatment of osteoarthritis.
- Acetaminophen generally is considered safe, although it may pose risks to the kidneys or to the liver in some individuals with liver disease.
- Aspirin is a popular medicine for many arthritic disorders because of its ability to relieve pain as well as inflammation (swelling, redness). However, aspirin is not suitable for people who have had a stomach ulcer or aspirin allergy.
Nonsteroidal anti-inflammatory drugs (NSAIDs) relieve pain as well as inflammation. There are a wide variety of both OTC and prescription NSAIDs to choose from, including:
- Diclofenac (Cataflam®, Voltaren®)
- Diflunisal (Dolobid®)
- Etodolac (Lodine®)
- Flurbiprofen (Ansaid®)
- Ibuprofen (Advil®, Motrin®)
- Indomethacin (Indocin®), Tolmetin (Tolectin®)
- Ketoprofen (Actron®,
- Meclofenamate (Meclomen®)
- Nabumetone (Relafen®)
- Naproxen (Aleve®, Anaprox®, Naprelan®, Naprosyn®)
- Orudis®, Oruvail®)
- Oxaprozin (Daypro®)
- Phenylbutazone
- Piroxicam (Feldene®)
- Salsalate (Disalcid®)
- Sulindac (Clinoril®)
Unfortunately, NSAIDs have been characterized as having a ‘double-edged sword,’ since gastrointestinal (GI) complaints – which range from stomach upset to ulceration and bleeding – are common side effects of these medicines.
- Such complaints sometimes can be controlled by taking the NSAID with food or by using antacids between meals.
- However, if GI problems are more than mild or are long-lasting, the physician may prescribe an NSAID that causes fewer GI side effects (for example, salsalate).
- Note that NSAIDs also can cause kidney damage, worsen blood pressure (with salt and fluid retention), and contribute to bleeding by affecting the platelets (clotting elements in the blood).
NSAID partners may be prescribed by a physician to lessen the side effects of NSAIDs. These include:
- Antacids
- The prostaglandin analoguemisoprostol (Cytotec®)
H2-blockers such as ranitidine (Zantac®)Proton-pump inhibitors such as omeprazole (Prilosec®).
The proton pump inhibitors and misoprostol decrease the risk of ulcers, while the H2-blockers only help symptoms.
Cox II inhibitors are reasonably new medications that reduce the pain of osteoarthritis and also reduce the chance of developing ulcers, and so partially preventing the GI complaints associated with NSAIDs. These medicines, which are available by prescription only, include:
- Celecoxib (Celebrex®)
- Rofecoxib (Vioxx®)
Vioxx was withdrawn from the market during September 2004 due to side effects that had not previously been anticipated at the time of its release just a few years earlier. These side effects include the increased risk of developing a stroke.
|
Nice To Know: Researchers have discovered two cyclooxygenase (“COX”) enzymes within the body:
Current NSAIDs inhibit both enzymes. Since inhibition of COX-1 leaves the stomach lining vulnerable, NSAIDs may promote side effects such as stomach ulcers and bleeding. By contrast, inhibition of COX-2, while providing pain relief, is less like to cause stomach ulcers or bleeding. COX-2 inhibitors – a new class of medications – was developed to manage the pain and inflammation of arthritis with the intention of preventing the negative side effects of NSAIDs. Two products, Celebrex® and Vioxx®, were approved by the U.S. Food and Drug Administration (FDA) in 1999 and became the most used of the anti-inflammatory medications. Unfortunately Vioxx® was found to have previously unrecognized and very significant unanticipated cardiovascular side effects, including increased risk of developing a stroke or a heart attack and was withdrawn from the market in September of 2004. Celebrex® (celecoxib) remains available. |
Muscle relaxants sometimes are prescribed for osteoarthritis if muscle spasms contribute to a person’s discomfort. These include:
- Cyclobenzaprine (Flexeril®)
- Carisoprodol (Soma®)
- Methocarbamol (Robaxin®)
Other prescription drugs, including sleep medications and antidepressants, may be beneficial in certain individuals.
Over-the-counter (OTC) creams, rubs, and sprays can be applied topically (to the skin) for temporary relief of pain in a sore muscle or joint. These products work in various ways, depending upon their ingredients. Some products contain:
- Salicylates (aspirin-related compounds that relieve pain)
- Skin irritants (chemicals that cause cold, warm, or other sensations, thereby reducing feelings of pain)
- Capsaicin (a “hot” substance found in chili peppers which blocks pain signals to the brain)
Most creams, such as those containing capsaicin, must be reapplied three to four times daily and may require two to four weeks of use before effects are noticeable.
Most programs that include medications emphasize the importance of:
- Sticking with a schedule for medication
- Taking only the medication prescribed or recommended by a physician
- Consulting a physician before taking any new medications, including over-the-counter (OTC) products. Some OTC products have the same ingredients as prescription medications, so one runs the risk of overdose unless all medications are discussed with a physician
|
Nice To Know: Q: My stomach is easily upset. Will arthritis medicine upset my stomach or give me an ulcer? A: Make sure that your physician is aware of your stomach problems so that he or she can prescribe a pain reliever that does not irritate the stomach or cause bleeding from or ulcers in the stomach, which these medications can sometimes do. Suitable choices may be an aspirin-free pain reliever, such as acetaminophen, or an NSAID that causes fewer GI symptoms. As an alternative, the physician may prescribe an additional medication to lessen the side effects of NSAIDs. It also may be beneficial to switch to the new COX-2 inhibitors that significantly lessen the chance of stomach problems |
Other Pain Relief Options
- Transcutaneous electrical nerve stimulation (TENS) is a technique that directs small pulses of electricity to specific nerves. The aim is to reduce the sensitivity of nerve endings in the spinal cord, thereby closing the pain “gates.” Although TENS is not effective in all arthritis sufferers, some people find it to be a practical means of pain control. The procedure, which produces a tingling sensation at the site of the electrical pads, has few side effects (some people have reported allergic reactions to the jelly used to apply the pads). TENS instruction usually is provided by a physiotherapist, who can explain how to position the pads, select the correct electrical frequency and pulse strength, and time how long the treatment should last.
Acupuncture may provide short-term relief of pain. If performed properly with sterile needles, acupuncture can do no harm. Acupuncture therapy is believed to work by stimulating the body’s own pain-relieving hormones. However, acupuncture cannot “cure” arthritis; its effects are temporary.- Therapeutic massage
- Yoga
- Physical therapy
Stress Control
Emotional stress sometimes causes arthritic symptoms to worsen. Repeated daily stresses – such as money problems, traffic jams, or shopping difficulties – may increase joint discomfort.
Although emotional anxiety does not appear to be as important a factor in osteoarthritis as it is in rheumatoid arthritis, osteoarthritic pain may develop after stressful life events, like the loss of a loved one or separation from a spouse.
Arthritis itself is a source of stress.
- Individuals may feel trapped in a vicious cycle in which arthritic pain causes stress and stress causes more pain.
- In addition, they may have a low self esteem and feel a loss of control because of arthritis-related concerns such as pharmaceutical bills, side effects from medicines, limited mobility, or unwelcome physical changes.
Stress management techniques are especially significant, because they can help people to regain a sense of control while relieving their arthritic pain.
Proven techniques for stress management include:
- Muscle relaxation
- Controlled breathing
- Biofeedback
- Self-hypnosis
- Time management
- Social support
- Assertiveness training
- Coping skills training
|
Nice To Know: Q: Will moving to a different climate improve my osteoarthritis? A: It is well known that arthritis sufferers often feel more joint pain in damp locations, just before it rains, or sometimes during humid periods. However, OA occurs in all climates. The effect of the weather really is a temporary effect on symptoms and does not actually affect the disease. This means that climate does not improve or worsen arthritis, although it may affect the symptoms. |
Injections Into The Joint
- Unfortunately, corticosteroids can cause adverse side effects (such as joint degradation) when injected indiscriminately over long periods of time directly into a joint. Therefore, they should be used only to treat occasional bouts of joint pain and swelling in OA, particularly in younger people.
- A single injection may be sufficient to relieve OA for several months. The effect lasts for different amounts of time in different people.
- They don’t work for everyone
Injectable
- Hyaluronic acid is a lubricating substance that is found in the normal joint fluid. If, as in osteoarthritis of the knee, inflammation breaks down hyaluronic acid within the joint, then lubrication is lost.
- Hyaluronic acid injection does not cause the side effects of most oral pain relievers. Therefore it is suitable for people who still suffer discomfort after being treated by pain medication, exercise, or physical therapy.
- Hyaluronic acid injection may provide relief for up to 12 months, but there is no indication that the treatment alters the progression of arthritis.
- Ongoing studies are investigating whether this method is effective for the shoulders and hips, but, to date, there is little information on the long-term effects of hyaluronic acid injection.
- In general, the treatment is well tolerated, and allergic reactions are rare.
Surgery
Although recent advances in joint surgery have improved the lives of millions of people throughout the world, surgery is NOT the first line of treatment for osteoarthritis.
|
Nice To Know: Surgery Surgery is reserved for people who have
|
Before surgery is ever contemplated, simpler treatments must be tried. Moreover, most surgeons prefer not to perform operative procedures in younger people unless their quality of life is severely affected by arthritis.
When surgery is necessary, it is performed by an orthopedic surgeon – a specialist in surgery of the bones and joints.
There are four main types of surgery available:
- Fusion (permanent joining of the bones in a joint, preventing motion)
- Osteotomy (realigning the joint)
- “Scoping” the joint (washing out the joint)
- Joint replacement (replacement of a damaged joint with an artificial joint)
- Fusion of the joint, otherwise known as
arthrodesis is a procedure in which the surfaces of the joint are removed and the bone ends are united. This provides pain relief and stability, but the joint cannot bend.Lack of mobility is a serious disadvantage of this procedure. Nevertheless, this is the preferred surgery for some younger individuals who have a single involved joint. Mobility in the other joints often will compensate for the loss of movement in the fused joint. The joints most commonly fused are smaller joints, such as those in the toes or fingers.
Younger people with severe arthritis of the hip or knee in whom fusion was once offered, are now considered for total
joint replacement (see below), though depending on the individual, a fusion may sometimes be preferable Osteotomy is an operation in which the surgeon cuts the bone below the affected joint, realigns it, and resets it in a better position. This procedure changes and improves the contact between the remaining healthy areas of cartilage in the joint. Afterwards, the painful areas do not rub against each other.Osteotomy provides pain relief and leaves the joint mobile; however, it can only be performed in a joint that is not already stiff. Osteotomy usually is reserved for joints with uneven damage. It is not performed frequently, although the procedure sometimes is a good choice for younger arthritis sufferers, since it can prevent further joint damage and postpone the need for joint replacement surgery. (For example, osteotomy of the tibia [shinbone] is performed to correct curvature and weight-bearing in the lower leg of adults with OA of the knee.)
- “Scoping” the joint is an expression used to describe
arthroscopy – the examination of the inside of a joint using a device equipped with a tiny video camera. By means of arthroscopy, the physician can look for damaged tissue directly within the joint.A small incision is made through the skin alongside the affected joint. Then, microsurgical tools are used to remove areas of cartilage or cartilage fragments that are causing irritation and thoroughly wash out the joint. Arthroscopy is an outpatient procedure and does not require an overnight stay in the hospital.
Joint “scoping” may provide temporary relief from symptoms – especially those caused by cartilage tears or particles; however, it does not stop the progression of osteoarthritis. It may help for a month in some, six months or much longer in others, and sometimes not at all.
- Total joint replacement involves the complete removal of the painful joint, which is exchanged for a man-made appliance. The artificial joint can be fashioned from a combination of materials, including stainless steel, Vitallium™ (a cobalt-chromium alloy), titanium, and high-density polyethylene plastic. Silicone rubber occasionally is used for joint replacements (hand, base of the thumb), if the surgeon elects not to fuse the joint.
The hip and knee have shown the greatest successes of all joint replacement surgery. Over 90 percent of people are free of pain and have good mobility following hip replacement surgery for osteoarthritis. Other joints that are less commonly replaced are the shoulder and elbow.
Unfortunately, joint replacements tend to last only 10 to 20 years. But another replacement generally can be performed, if needed. This repeat surgery is called a revision.
For further information about hip replacement, go to Total Hip Replacement.
For further information about knee replacement, go to Total Knee Replacement.
|
Nice To Know: I have osteoarthritis in my hip joint. Will I need surgery to correct it? A: Very likely, no. Most people with osteoarthritis never need to have surgery. Surgery only becomes an option if the person suffers from
Simpler treatments must always be tried before surgery is considered. |
Living With Osteoarthritis
Even after a diagnosis of osteoarthritis, individuals can continue to lead a full and active life.

In addition to various self-treatments such as exercise and medical treatments such as injections into a joint, other measures can be taken to live with OA. These measures include:
- Joint protection
- Assistive devices
- Help from healthcare professionals
- Developing a self-management program
By learning about osteoarthritis and educating oneself about its treatment, an individual can improve his or her lifestyle and have a new sense of purpose. Your physician is a helpful resource.
Some individuals explore other treatments, including unproven “remedies.” While some of these options are safe, others can cause harm. It’s prudent to explore the facts and risks before trying such options.
Joint Protection
Joint protection begins with learning new ways to use the arthritic joint. Joint stress and strain can be limited by following a few simple rules.
For the upper body joints:
- Avoid overburdening small and weaker joints by using larger joints to carry heavy things. For example, carry shopping bags using the forearms or palms of the hands, rather than the fingers.
- Avoid neck strain by placing reading material or work objects at eye level. Don’t look up or down for long periods of time.
- Relieve finger joint strain by using extra-thick pens when writing.
- Wear thick gloves to reduce joint strain when a tight grip is needed to hold a tool, heavy pot, or other object.
- Increase leverage by using long-handled tools and reaching devices when performing activities such as gardening, housework, and retrieving objects from high places.
For the lower body joints:
- Bend at the knees and straighten the legs (while keeping the back straight) to lift objects from the ground if back pain is a problem.
- Get up from a chair by sliding forward to the chair’s edge, keeping the feet flat on the floor, and using the palms of the hands to push against the chair’s arms or seat. Stand up by straightening the hips and knee. Use higher seats rather than deep, soft sofas.
- Never squat or kneel, as these positions strain the hips and knees.
- Maintain good posture to avoid putting stress on the joints.
- Wear well-cushioned athletic shoes with good arch support whenever possible. If dress shoes must be worn, women should choose styles with heels that are no higher than one inch. Men should choose lace-up rather than slip-on styles, which provide less support.
- Use support devices(cane, walker) if necessary, to reduce strain on the hips and knees when walking. A cane should be held in the opposite hand to the hip or knee affected.
Assistive Devices
Assistive devices can help people with arthritis to perform everyday tasks. Such devices include:
- Canes, walkers, and other walking aids
- Cervical collars
- Special pillows
- Back braces and supports
- Splints
- Jar openers
- Faucet turners
- Door knob turners
- Footstools
- Key turners
- Writing devices
- Reaching devices
- Shoe inserts
- Bookstands
- Bathroom equipment (such as raised toilet seats, handrails by toilet and shower)
Many of these devices – such as splints used to rest sore joints – should be prescribed by a physician and fitted by an expert.
|
Nice To Know: |
|
|
Assistive Device Manufacturers |
|
|
Company Name |
Product Line |
|
D’MANNCO, INC. |
Manufacturers of Pucci® Air orthotic products, which use a patented air inflation system to apply low stretch therapy. For treatment of fingers, hands, elbows and knees in adults and children |
|
DYNATRONICS CORPORATION Internet address: www.dynatronics.com |
Offers a full line of orthopedic assistive and supportive devices, including cervical pillows and collars, lumbar supports and cushions, and neck supports. |
|
FLA ORTHOPEDICS Internet address: www.flaorthopedics.com |
Offers a full line of orthopedic, sports medicine, and occupational supports as well as bracing and fracture management products. |
|
GENDRON INC. Internet address: www.gendroninc.com |
Specializes in bath safety products for people who are overweight |
|
GENERATION I USA, INC. Internet address: www.gen2.com |
Pain relief products. Custom and off-the-shelf osteoarthritis and ligament knee braces |
The above products are listed for informational purposes only. Endorsement is not implied.
Help From Healthcare Professionls
In addition to family physicians, internists, and rheumatologists (specialists in connective tissue disorders), many other healthcare professionals are available to help arthritis sufferers who have difficulties performing everyday activities. Such individuals are, in fact, essential to a comprehensive arthritis treatment plan. They include:
- Physical therapists and physiatrists
- Occupational therapists
- Nurses
- Pharmacists
- Dietitians
- Psychiatrists and psychologists
- Social workers
Physical therapists and nurses often have solutions for problems with daily activities (walking, dressing, climbing stairs, bathing), and they can offer ways to cope with disability. In addition, they can provide instruction about joint protection and suggest appropriate aids and assistive devices protection.
Occupational therapists are able to assess the home and recommend changes that can make it safer, more comfortable, and easier to get around.
Psychiatrists, psychologists, and social workers can help individuals to cope with stress, and they can advise both patients and families about the emotional adjustments needed for the new circumstances presented by arthritis.
|
Nice To Know: Researchers are investigating whether chondroitin sulfate or glucosamine sulfate can be beneficial in the treatment of osteoarthritis Chondroitin sulfate is the synthetic form of chondroitin Glucosamine is the synthetic form of glucosamine Chondroitin and glucosame are substances naturally found in connective tissue such as |
Developing A Self-Management Program
Self-management is perhaps the most significant factor in controlling osteoarthritis. A person who anticipates problems and makes lifestyle changes is better able to achieve control. In addition, sharing information with a physician will help to thwart potential difficulties and make the most of available treatments.
Arthritis education is key. Many programs are available through the Arthritis Foundation and other resources. For the best results, it is advisable to learn:
- Symptom management skills to lessen pain by exercising, using heat or cold, or other strategies.
- Coping skills to help contend with the arthritis-related changes, including changes in appearance, mood, or levels of pain and stress.
- Activity planning, so that if symptoms are problematic, activities are planned for the best times or days.
Another simple but effective tool is a personal journal. A small book or log can be used to record both good and bad responses to treatment. The journal can be brought to a physician and reviewed. In this way, the person and his or her physician can both cooperate in the treatment program and overcome any problems that may arise.
In addition, a journal can help to reveal the progress that is made when one sticks with a treatment program. Individual achievements may be small, but they can add up to significant changes over time. To make the most of a journal, a person should note weekly:
- Exercise periods
- Joint protection strategies
- Beneficial dietary changes
- Methods used to cope with pain and stress
- Attendance at arthritis classes
|
How-To Information: Create an Arthritis Journal Here is an example of how a personal journal could look: PERSONAL JOURNAL Month: _____________________ |
||||||||
|
MON. |
TUE. |
WED. |
THU. |
FRI. |
SAT. |
SUN. |
MIN. PER WEEK |
|
|
WEEK 1 Exercise Joint Protect. Diet Coping Classes/Groups |
|
|||||||
|
Responses (good/bad) |
||||||||
|
WEEK 2 Exercise Joint Protect. Diet Coping Classes/Groups |
||||||||
|
Responses (good/bad) |
||||||||
|
WEEK 3 Exercise Joint Protect. Diet Coping Classes/Groups |
||||||||
|
Responses (good/bad) |
||||||||
|
WEEK 4 Exercise Joint Protect. Diet Coping Classes/Groups |
||||||||
|
Responses (good/bad) |
TOTAL |
|||||||
Unproven “Remedies”: Know The Risks
Unproven arthritis remedies are treatments that have NOT been:
- Evaluated by controlled scientific studies, or
- Proven effective or safe when evaluated by controlled scientific studies
In order to be accepted by the medical community, all medicines and medicinal aids must undergo numerous tests. Such tests must demonstrate that the products are effective in repeated controlled studies. Arthritis remedies, in particular, must show that they are able to accomplish goals such as pain relief, reduction of inflammation, or improvement in joint function.
Tests also must verify that the product is safe, since high frequencies of unwanted side effects limit the usefulness of any treatment. According to a recent survey by the U.S. Department of Health and Human Services (USDHHS), one in 10 people who have tried unproven arthritis remedies report harmful side effects.
Yet even if an unproven remedy is harmless, it can still have a negative effect if it causes a person to delay or stop using proven arthritis treatments that were prescribed by a knowledgeable physician.
- Sometimes an individual may believe that an unproven remedy is effective simply because the remedy was used when symptoms were going into a natural remission (temporary lessening of symptoms).
- In addition, disease improvement due to positive thinking – otherwise known as the “
placebo effect” – may temporarily relieve symptoms in some people. Unfortunately, such improvement usually is short-lived, while the underlying arthritis progressively worsens.
|
How-To Information: Unproven Remedies for Arthritis Unproven but harmless remedies include:
Unproven and potentially dangerous remedies include:
|
Osteoarthritis: Frequently Asked Questions
Here are some frequently asked questions related to osteoarthritis.
Q: Will a change of diet improve my osteoarthritis?
A: Research does not indicate that modifying one’s diet or eating larger amounts of certain foods will prevent OA or reverse its effects. Yet it is prudent to control obesity by limiting calories, opting for healthy eating habits, and cutting down on the intake of fatty foods. Some changes in body chemicals related to painful inflammation can be initiated by replacing red meats with fish and by using certain vegetable oils. Some people believe that ‘acid foods’ cause arthritis. This is not the case. In addition, alcohol does not affect OA, although alcoholism can damage bone and be a secondary cause of OA.
Q: I have broken my knee twice playing football. Will I develop osteoarthritis in that joint?
A: It is possible. Joint trauma is known to be a factor in the development of OA. Furthermore, if a bone is broken near a joint, there is a greater likelihood of developing OA in the joint itself.
Q: My stomach is easily upset. Will arthritis medicine upset my stomach or give me an ulcer?
A: Make sure that your physician is aware of your stomach problems so that he or she can prescribe a pain reliever that does not irritate the stomach or cause bleeding from or ulcers in the stomach, which these medications can sometimes do. Suitable choices may be an aspirin-free pain reliever, such as acetaminophen, or an NSAID that causes fewer GI symptoms (such as salsalate). As an alternative, the physician may prescribe another medication to lessen the side effects of NSAIDs. It also may be beneficial to switch to the new
Q: Will moving to a different climate improve my osteoarthritis?
A: It is well known that arthritis sufferers often feel more joint pain in damp locations, just before it rains, or sometimes during humid periods. However, OA occurs in all climates. The effect of the weather really is a temporary effect on symptoms and does not actually affect the disease. This means that climate does not improve or worsen arthritis, although it may affect the symptoms.
Q: I have osteoarthritis in my hip joint. Will I need surgery to correct it?
A: Very likely, no. Most people with osteoarthritis never need to have surgery. Surgery only becomes an option if the person suffers from (1) severe pain that is not relieved by available treatment methods, (2) a dramatically impaired ability to perform daily activities, or (3) marked joint instability. Simpler treatments must be tried before surgery is considered.
Q: Both my mother and father had osteoarthritis. Am I likely to get it too?
A: Heredity appears to play a role in osteoarthritis, although the exact causes remain unknown. In a few people scientists have found an abnormal gene that causes the early breakdown of joint
Osteoarthritis: Putting It All Together
Here is a summary of the important facts and information related to osteoarthritis.
- Osteoarthritis is a degenerative condition that develops when
cartilage – the lining tissue that cushions the ends of the bones in a joint – breaks down. This can happen because of prolonged wear-and-tear, prior injury, or because the cartilage is genetically weak or altered by other disease. - Osteoarthritis typically strikes the hands, and the weight-bearing joints (knees, hips, backbone, feet).
- The cause(s) of osteoarthritis remain unknown; however, certain factors are associated with OA, such as joint wear-and-tear, joint injury or overuse, inactivity, excess body weight, and heredity.
- Many people don’t realize that they have OA, because they are free of symptoms. If symptoms are present, they may include joint pain, limitation of motion, stiffness after inactivity, and bony enlargement (“
spurs “). - The treatment of OA should be tailored to meet the needs of the individual. It usually begins with a comprehensive program that emphasizes proper exercise, diet and nutrition, joint protection techniques, coping skills for pain and stress, self-management, and medication.
- Surgery is NOT the first line of treatment for osteoarthritis. It is reserved for people who have severe pain that is not relieved by available treatment methods, marked joint instability, or a significantly impaired ability to perform daily activities due to pain and loss of mobility.
- Unproven arthritis “remedies” are treatments that have NOT been evaluated by controlled scientific studies, or proven effective or safe when evaluated by controlled scientific studies.
- Although arthritis has become a leading cause of disability in the United States, it can be managed successfully. Healthcare professionals who are available to help coordinate OA treatment programs include family physicians, internists, and rheumatologists (specialists in connective tissue disorders), physical therapists and physiatrists, occupational therapists, nurses, pharmacists, dietitians, psychiatrists and psychologists, and social workers.
Osteoarthritis: Glossary
Here are definitions of medical terms related to osteoarthritis.
Acupuncture: Ancient Chinese technique that uses needles to pierce specific areas of the body along nerve pathways. Acupuncture may be used to relieve pain, induce anesthesia, or serve as a treatment for certain diseases.
Arthrodesis: Surgical fusion of a joint. The joint becomes stiff after the surfaces of the joint are removed and the bone ends are united.
Arthroscopy: “Scoping a joint.” The examination of the inside of a joint using a device equipped with a tiny video camera.
Bouchard’s nodes: Bony spurs that occur on the middle finger joints.
Cartilage: Fibrous, flexible connective tissue that cushions the ends of the bones within the joints and serves as a framework for bone development in the fetus.
Collagen: A protein that makes up the white fibers of connective tissue, such as cartilage.
Corticosteroids: Medications (e.g., prednisone) that are related to cortisone, a naturally occurring hormone. Corticosteroids lessen inflammation, swelling, and pain. In some cases, corticosteroids are injected directly into a joint; however, they can have serious side effects – such as damage to bones and cartilage – especially when used over long periods of time.
COX-2 inhibitors: New class of medications that were developed to manage the symptoms of arthritis without negative gastrointestinal effects. COX-2 inhibitors stop the activity of specific cyclooxygenase (“COX”) enzymes, which release the substances (prostaglandins) responsible for pain and inflammation.
Dimethyl sulfoxide (DMSO): Solvent (liquid capable of dissolving things) that easily penetrates the skin. It is a dangerous, unproven “remedy” for the pain and inflammation of arthritic disorders.
Fibromyalgia: Disorder (also known as fibromyositis or tension myalgia) that primarily affects muscles and their attachments to bone. It does not cause joint deformity. Fibromyalgia is characterized by general muscle pain, stiffness, fatigue, sleeplessness, and numerous tender points at the sites where muscles join to bones.
Genes: Biologic units of heredity that are located at a specific position on a particular chromosome (cell structure composed of a linear thread of genetic material).
Gout: Inherited disorder (also known as crystalline arthritis) that is characterized by a variable level of uric acid (a normal byproduct of foods) in the blood and sudden severe arthritis due to crystal deposits (sodium urate) within the joints.
H2-blockers: Chemicals that block the activity of histamine, which is a powerful stimulator of gastric acid production. Ranitidine (Zantac®) is a well known H2-blocker.
Heberden’s nodes: Bony spurs that occur on the end joints of the fingers.
Human leukocyte antigens (e.g., HLA-DR4 and HLA-DR1): Tissue-specific ‘marker’ proteins (HLA proteins) that are found on the surface of some cells, such as leukocytes (white blood cells). These proteins correspond to the HLA genes that are located on chromosome 6 in humans.
Hyaluronic acid: Lubricating substance that is found in the normal joint fluid. Injectable hyaluronic acid – which currently is marketed under the brand names Hyalgan® and Synvisc® – is a new FDA-approved treatment for osteoarthritis of the knee
Joint replacement: Complete surgical removal of a painful joint, which then is exchanged for a man-made appliance.
Nonsteroidal anti-inflammatory drugs (NSAIDs): Medications that are often used to relieve the symptoms of osteoarthritis. NSAIDs reduce the pain and swelling associated with inflammation. The most commonly used NSAIDs are aspirin, ibuprofen, and naproxen.
Osteoporosis: Disorder in which bones and skeletal tissues become less dense and break easily. Osteoporosis occurs most often in post-menopausal women and elderly men.
Osteotomy : The cutting of a bone. More specifically, an operation in which the surgeon divides the bone below the affected joint and allows it to heal in a slightly altered position. The bone is realigned, with improved contact between the remaining healthy areas of cartilage in the joint.
Placebo: A medically inactive substance that is used in controlled studies to determine the effectiveness of a test drug. Placebos have been shown to lessen symptoms in some people, most likely because of the individual’s positive attitude about treatment.
Prostaglandin analog: Chemical that functions like a prostaglandin – any of a group of fatty acid substances that perform a variety of functions within the body, including control of inflammation and blood vessel permeability and regulation of hormones, stomach acid secretion, body temperature, and smooth muscle contraction (for example,misoprostol [Cytotec®]).
Proton-pump inhibitors: Chemicals that suppress stomach acid secretion by inhibiting a specific enzyme system on the surface of the stomach’s parietal cells. This enzyme system is regarded as the acid (proton) pump within the stomach mucosa (for example, omeprazole [Prilosec®]).
Rheumatoid arthritis (RA): Disorder that is believed to result from an “autoimmune” process in which the body’s immune system attacks itself. It is a system-wide disease that usually last for many years. In some patients, RA affects such organs as the heart, lungs, and eyes. Patients with active RA often feel feverish or ill.
Rheumatoid factor (RF): Protein (immunoglobulin M, IgM) found in the blood of most people with rheumatoid arthritis.
Spurs: Osteoarthritic condition in which bony growths project outward from the ends of a bone in a joint.
Synovial fluid: Thick, clear fluid produced by the synovial membrane and found in joint cavities.
Synovial membrane: Inner, smooth lining of the joint cavity.
Systemic lupus erythematosus (SLE): Inflammatory connective tissue disorder with variable features, including fever, fatigue, arthritis and joint pain, and red skin lesions on the face, neck, and/or upper limbs.
Transcutaneous electrical nerve stimulation (TENS): Technique that directs small pulses of electricity to specific nerves. The aim is to reduce the sensitivity of nerve endings in the spinal cord, thereby closing the pain “gates.”
Osteoarthritis: Additional Sources Of Information
Here are some reliable sources that can provide more information on osteoarthritis.
Arthritis Foundation Services
Arthritis Foundation(national office)
Phone: 800-283-7800
http://www.arthritis.org
- Arthritis Self-Help Course (ASHC)
A 6 week [15-hour] class that teaches people how to take control of their own care.
- Bone Up on Arthritis (BUOA)
A simplified, self-paced arthritis course. Six lessons on audiocassettes and a workbook provide helpful information about arthritis management.
- Arthritis Foundation YMCA Aquatics Program (AFYAP)
- A 6- to 10-week warm water exercise class that is conducted in a heated pool. AFYAP is designed for people with impaired joint motion and strength. It focuses upon muscle strengthening and joint mobility.
- Land Exercise Arthritis Program (LEAP), and People with Arthritis Can Exercise (PACE)
Courses that offer several levels of exercise to benefit people with any type of arthritis.
- Joint Efforts
A program for older adults that helps to explain the principles of joint protection.
- In Control®
A self-paced videotape about arthritis (text and audiocassette supplements are available).
- Arthritis Home HelpTM
An individualized, computerized, self-management plan that uses quarterly questionnaires, self-care books, and tapes.
- Arthritis Today magazine
An award-winning, bimonthly magazine (with $20 membership donation). For instant membership, call toll-free:(800) 933-0032.
Other Arthritis Foundation Services
- Local Arthritis Foundation Chapters (these may provide a selection of support groups and clubs)
- Arthritis specialist list
- Educational brochures
- One-session educational meetings
Other Support Group Sources
- The Internet
- YMCA and YWCA
- Social service agencies
- Hospital outreach programs
- Senior clubs
- Health clubs
- Surgical supply stores and catalogues
Helpful Websites
American College of Rheumatology (ACR)
http://www.rheumatology.org/
American Academy of Orthopedic Surgeons
www.aaos.org
The Arthritis and Glucosamine Informaion Center
www.glucosamine-arthritis.org
Books
Arthritis: A Comprehensive Guide to Understanding Your Arthritis, by James F. Fries, M.D., is recommended by the Arthritis Foundation as a reference for its trainers and teachers. (5 rating)